
BLOG

The Top 10 Subconscious Blocks to Success in High Achievers
When you imagined your future…
You imagined pretty much what you have now: A high-powered job, a great spouse, a couple of kids, a dog, a fancy car(s), a nice house on the water, and vacations to cool places like Iceland and Hawaii. It’s not so much that your life LOOKS different than you imagined on the outside, it’s that it FEELS different on the INSIDE.
The Top 10 Subconscious Blocks to Personal Success in High Achievers
When you imagined your future…
You imagined pretty much what you have now: A high-powered job, a great spouse, a couple of kids, a dog, a fancy car(s), a nice house on the water, and vacations to cool places like Iceland and Hawaii. It’s not so much that your life LOOKS different than you imagined on the outside, it’s that it FEELS different on the INSIDE.
It doesn’t feel fulfilling. It doesn’t feel carefree. It doesn’t feel enjoyable. In fact, it doesn’t feel like much of anything, except a massive burden. And, because of that you feel resentful and angry.
You also feel guilty for being unhappy because you have so much more than other people do. You have everything you wanted. You SHOULD be happy. What the fuck is your problem? Mommy and daddy didn’t love you enough? Jesus. You feel like maybe you should stop being such a fucking cliché and just get over it already. The problem is, you can’t. You’ve tried. Now, you’re a functioning alcoholic-workaholic.
What got in the way…
So, what’s your problem?
How much time do you have? The list is long.
The top 10 subconscious blocks to personal success in high achievers
1) Trust: Trust is a big issue. You don’t trust others and you don’t trust that god/source/universe actually gives a shit about you, so basically this means that you only have yourself to rely on. But, you don’t trust yourself either, so you’re pretty much screwed.
2) Honesty: It’s not so much that you are dishonest, it’s more that you are pretending. You don’t necessarily mean to deceive others, you just don’t want them to see the real you because if they did, they wouldn’t like what they saw. So, you wear a mask that gives people what you think they want.
And, truth be told, you’ve been at this charade for so long that you don’t even know who the real you IS. All you know is that you’d like to stop pretending and get honest because this charade is exhausting.
Want more? Get the full, free guide to the top 10 subconscious blocks to success by clicking below.

Gaslighting & Intuition Guide: What gaslighting is, how to respond, how it damages intuition and methods for intuition repair
Click the button below to get the guidebook on gaslighting and intuition.

Are we sabotaging our dream lives, and humanity in the process? Getting over our egos by evolving our consciousness, and saving humanity in the process. A manifesto.
“Until we have met the monsters in ourselves, we keep trying to slay them in the outer world. And we find that we cannot. For all darkness in the world stems from darkness in the heart. And it is there that we must do our work” (Williamson, 2002, p. 13).
Are We Sabotaging Our Dream Lives, and Humanity in the Process?
In short: Yes. But, usually not purposely. Sabotage happens unconsciously because old stories, beliefs, fears and wounds are still running the show, outside of our conscious awareness. These old stories, beliefs, fears and wounds come from our individual experiences, our families (including their genes) and the outside world.
We are only consciously aware of an infinitesimal amount of what is actually happening in our minds and environment (we take in 11 million bits of information each second but only consciously process 40 of these; Zimmerman, 1986). And if we are only aware of a small fraction of what is happening, that means we only have control over a small fraction of what is happening. This is fairly disconcerting, especially for those of us who like certainty and control. The good news is that we can use various tools to begin to become consciously aware of that which was previously unconscious. Therapy or healing work, meditation, dream interpretation, inner child work, energy healing, self-reflection and introspective writing (journaling) can all help unearth these unconscious processes, so we can begin to take back control of our lives. However, as anyone who has attempted self-improvement can attest, the moment we try to make a change, we get pushback, from external forces (e.g., the culture) and internal forces (e.g., the ego). Our self-improvement is a threat to the status quo of the culture and our ego. As a result, these forces will try to step in to sabotage our efforts. It’s our job to stay strong and keep fighting for change.
Are we sabotaging our dream lives, and humanity in the process? Getting over our egos by evolving our consciousness, and saving humanity in the process. A manifesto.
Brianna D. Mann, Ph.D.
“Until we have met the monsters in ourselves, we keep trying to slay them in the outer world. And we find that we cannot. For all darkness in the world stems from darkness in the heart. And it is there that we must do our work” (Williamson, 2002, p. 13).
Are We Sabotaging Our Dream Lives, and Humanity in the Process?
In short: Yes. But, usually not purposely. Sabotage happens unconsciously because old stories, beliefs, fears and wounds are still running the show, outside of our conscious awareness. These old stories, beliefs, fears and wounds come from our individual experiences, our families (including their genes) and the outside world.
We are only consciously aware of an infinitesimal amount of what is actually happening in our minds and environment (we take in 11 million bits of information each second but only consciously process 40 of these; Zimmerman, 1986). And if we are only aware of a small fraction of what is happening, that means we only have control over a small fraction of what is happening. This is fairly disconcerting, especially for those of us who like certainty and control. The good news is that we can use various tools to begin to become consciously aware of that which was previously unconscious. Therapy or healing work, meditation, dream interpretation, inner child work, energy healing, self-reflection and introspective writing (journaling) can all help unearth these unconscious processes, so we can begin to take back control of our lives. However, as anyone who has attempted self-improvement can attest, the moment we try to make a change, we get pushback, from external forces (e.g., the culture) and internal forces (e.g., the ego). Our self-improvement is a threat to the status quo of the culture and our ego. As a result, these forces will try to step in to sabotage our efforts. It’s our job to stay strong and keep fighting for change.
Our Culture
Good lord, where do I begin? As we will discover throughout the journey of this article, humanity is in big trouble, on the brink, and a large part of this problem is the fact that, we are still very unevolved: socioculturally, psychologically, spiritually, educationally, economically, politically. Our collective consciousness level is dangerously low, evolving, but dangerously low. This is reflected in our cultural narratives (i.e., the stories that drive how we think, feel, speak and behave), the ways in which we relate to other people and our planet, the ways in which we try to solve social problems, how we write our laws, how we correct antisocial behavior, and ironically, in our attempts to evolve our consciousness (e.g., using methods like spiritual bypassing and toxic positivity). We are a culture that uses force to take what we want, shame and fear to manipulate change, and delusion to convince ourselves nothing is wrong. We are a culture that has forgotten how to love and how to dream.
Culture isn’t simply a sum of the parts, of the individual humans, it is a greater whole, an autonomous organism. It is an organism that has the same goal all organisms have, and that goal is survival. Culture seeks to maintain itself and in so doing, it seeks to eliminate any potential threats to its survival. Disruption of the cultural status quo through change, even positive change, is seen as a survival threat, so the culture acts accordingly, by attempting to eliminate the threat.
There are people among us who dream of a different world, who haven’t forgotten how to love, who seek to disrupt the status quo, but they are often overpowered by the might of the culture, their gentle voices silenced by the collective’s resounding cacophony. They try to make change but they are met with opposition at every turn. They are seen as a survival threat to the collective, so the collective will do whatever it takes to eliminate that threat. Surprisingly, these dreamers haven’t given up the fight. In fact, in the face of adversity, many of them just fight harder. And, as we’ll see when we discuss the recent increase in human consciousness, their efforts are gaining ground. But they need our help. As we go through this article, we will see that it is up to us as individuals to raise our energy levels, in order to raise the energy of the collective, so we can live in a better world and pull ourselves back from the brink of complete and utter destruction. But, in order to raise the energy of the entire collective, we must begin with our egos.
Our Egos
The ego is probably one of the most misunderstood aspects of the human psyche. It’s no wonder it has an inferiority complex, and feels the need to control every aspect of our lives. People often confuse “having an ego” with narcissism, an inflated and grandiose sense of self-importance. But, that’s not what having an ego means. That’s what having an inflated ego means. Psychiatrist Carl Jung conceptualized the ego as the conscious part of our mind, the part that represents our personal identity as a unique and separate being; the ego is the part that runs the show, makes decisions, organizes, navigates the concrete world, scans for danger and mitigates threats (Hopwood); and it is also the part that reminds us just how unique and special we are, sometimes to an inflated degree. We need our egos to stay alive and navigate this physical world. The problem is, our egos, ironically, take up too much space in our psyches, often functioning to our detriment. It is the ego that makes sure we continue to use our fear-based operating system (discussed below), even when it no longer serves us. Under the guise of protection, the ego ensures that we play it safe, small and status quo in this world. When we try to act in opposition to the ego’s wishes, the ego throws a temper tantrum and we are forced to either comply or deal with the consequences. The consequences are typically the felt senses of shame, fear, depression, self-loathing, self-doubt and self-deprecation. Most of us choose to comply in order to avoid these consequences.
Although the ego’s goal was initially preservation of the human whose body it resides in, it has, like the culture, mutated into a self-serving organism, sometimes to the detriment of the human. The ego now has one goal, self-preservation, and there is nothing it fears more than irrelevance, not surprisingly. So, the ego will do whatever it takes to ensure that it maintains employment as Supreme Ruler of the Psyche. However, as we will discuss throughout this article, relegation of the ego to a lesser role is exactly what we need at this point in our individual and collective evolutions.
Our Unconscious Operating System: Fear 1.0
What is important to understand is that for all living beings, the primary goal is survival. This goal is achieved using an operating system designed to mitigate threats and maximize conditions that facilitate survival. This system is the default operating system for all living beings, meaning it will run interminably on survival mode unless programmed to do otherwise. I like to call it, Fear 1.0. The commands Fear 1.0 can execute in humans are Fight, Flee, Freeze and Fawn. (For those of you not familiar with the Fawn command, it is the one that uses personal charm to increase rate of survival.) Although much of the functioning of this operating system is automatic and unconscious, the ego is the part makes sure it continues to run, interminably. This means that if we decide to do anything out of the ordinary, or god forbid, take a risk, the ego will step in to make sure nothing changes. The ego is like the operating system’s supervisor, one that insists upon micromanaging everything.
This operating system and these simple commands were helpful in the early stages of our evolution when resources were scarce, shelters were primitive, medicine was rudimentary, and predators roamed freely. Today, most of our challenges/threats come from within our psyches, homes and communities, from the greater sociocultural structure, and are chronic and often amorphous, rather than coming from external, acute, and tangible sources like wild animals, noxious plants, distant tribes and threatening weather conditions. Because Fear 1.0 is designed to work with the latter, it doesn’t work nearly as well to mitigate the types of threats we face in modern culture.
Modern-Day Threats to Survival
There are three primary areas from which modern-day survival threats emerge: Genetics, individual environment and the environment at large, including our communities, society, and the natural environment. Genetics can make us more prone to survival threats in and of themselves (e.g., through inheritance of a compromised immune system). Genetics can also interact with our environment to increase risks, as in the case of intergenerational trauma, where the effects of trauma repeat or otherwise impact subsequent generations, even going so far as to contribute to changes in the structure of our DNA itself. In other words, trauma experienced generations ago appears to be literally stored in the DNA of subsequent generations (Selimbasic, Sinanovic, & Avdibegovic, 2012; Snyder et al., 2016; Youssef, Lockwood, Su, Hao, & Rutten, 2018). Indeed, as described in Deuteronomy 5:9, the sins of the father will be visited upon the third and the fourth generations. This passage doesn’t simply refer to the sinful acts of the father, it refers also to intergenerational trauma; in other words, the sins inflicted upon the father (and mother) will be visited upon the third and fourth generations (Hollis, 2013; New International Version, 1978/2011). Even though these sins are not our own, it is our job to atone for them (by healing the wounds they have caused), if we wish to be free and if we wish for our children to be free.
Individual environmental threats to survival include the holy trinity of soul injury: abuse (physical, sexual and emotional-including psychological and verbal abuse), neglect (emotional and physical), and other traumas (e.g., combat trauma, car accidents, witnessing violence). Also included in the individual environmental threat category are bullying, poverty, parental addiction and mental health concerns, food scarcity, unstable or unsafe housing and social isolation (Centers for Disease Control and Prevention).
Survival threats that come from the environment at large, that come from community, societal, and natural environments, include racism and other forms of discrimination (e.g., sexism, classism, ableism, heterosexism), community violence, community-wide poverty, immigration, pollution, social and environmental disorder, easy access to drugs and alcohol, limited educational opportunities, high unemployment rates, natural disasters, and man-made disasters (e.g., chemical spills; Centers for Disease Control and Prevention; Felitti et al., 1998).
When Fear 1.0 tries to mitigate these modern-day threats to survival, using its original commands of Fight, Flee, Freeze and Fawn, it has limited success. This is because this system was designed to respond to acute, time-limited, external and tangible threats. Many of the threats we face in modern day are chronic; found within our bodies (e.g., our trauma wounds), families and communities; inescapable; amorphous (e.g., poverty, institutional racism, internalized misogyny); or are simply unresponsive to these commands. What we have done is to adapt our systems by developing certain behavioral patterns with governing belief systems, which are iterations of the original commands of Fight, Flee, Freeze and Fawn. These adaptations are called defense mechanisms and include options such as projection, reaction formation, denial, regression, repression, dissociation, avoidance, intellectualization, distraction, numbing, deflection, people pleasing and more. But like the original commands from which they are derived, these defense mechanisms aren’t effective solutions to the threats we face in modern-day society. In other words, our operating system, Fear 1.0, its commands and their modern-day adaptations, are no longer serving us. In fact, operating on our fear, defense, scarcity and power-based system is actually driving humanity to the brink of extinction because now, rather than fighting actual external threats, we have enlisted our defense mechanisms to inadvertently begin waging war in our own bodies and in our own backyards: We are now harming ourselves, harming the family and community systems that once protected us, and we are overtapping and overpowering (e.g., through development, deforestation, pollution, unsustainable agriculture, mining, drilling) Mother Earth’s natural ability to support us. We are now the biggest threats to our survival, our own worst enemy. It is self-evident that humanity needs a new operating system, needs to evolve in a new way, that humanity needs an evolution of consciousness.
Humanity on the Brink
When I’ve posed this problem and resultant solution to others, some say, “Hasn’t humanity always been on the brink of collapse? I feel like this has happened so many times and yet, we’ve always survived.” That is true. For having such a large and evolved cerebral cortex, we are really fucking stupid, and also, really fucking lucky. Each time we’ve been on the brink of collapse, or have experienced a small collapse, we’ve come back. But, that doesn’t mean we do nothing now. And, this time…well, this time our home planet is in jeopardy in a way that it’s never been during the Cenozoic Era. The current rate of extinction is comparable to the end of the Mesozoic (Reptilian) Era, and we all know how that turned out (Wilson, 2006). I guess we could tell ourselves that it’s going to be fine this time, but all of the experts are predicting that it most definitely is not going to be fine unless we take prompt and aggressive action, and even then, the next 30 years are going to be a complete shit show (Plumer & Fountain, 2021). I know that some people are holding out hope for the discovery of a new planet or perhaps a space station situation on Mars. But, if you watched Battlestar Galactica, 1) you’d understand how perilous that journey would be and 2), you’d understand that if we don’t learn our lessons now, we’ll just fuck up the next planet we inhabit and end up in the same predicament (Moore & Eick, 2004). In fact, this is one of the reasons why Europeans went searching for a new land. Medieval Europe’s forests, fields and streams had become so depleted and polluted, that they needed to find new ones to exploit (that, and the ruling class had begun to usurp the remaining land, resources and belief systems-sound familiar?). This quest led to some fairly significant human rights violations (e.g., genocide, enslavement, rape, pillaging, murder, torture, false imprisonment, ethnic and religious persecution) and only bought humanity about 500 years (Boissoneault, 2019; Olson-Raymer, 2014). Here we are again. So, I think it’s time we pull our collective head out of our collective ass, learn our lessons and do things differently this time around. Or, we could just give up and do nothing, which is what some people seem to have done. I mean, why bother?
So, you decide: Are you going to give up and do little to nothing as the planet becomes uninhabitable and humanity dies, or are you going to at least try to make a difference? Are you going to be complicit or are you going to rise up and do the difficult, but right thing?
It’s Time for an Evolution-Revolution.
The solution philosophers and spiritual leaders are proposing is what I mentioned before: an evolution of consciousness. There are a lot of great books explaining what an evolution of consciousness might look like. Three of my favorites are The Celestine Prophecy, The Big Leap and Power vs Force: The Hidden Determinants of Human Behavior. But let’s not stop there. My ego is inflated enough to believe that my field, the field of psychology, is going to help lead this evolution-revolution because we have what the world needs. And, what the world needs is for people to heal their wounds, let go of their need to overpower the environment and others to feel okay, and stop projecting their pain onto others and the planet. As they say, “hurt people, hurt people;” we can extend this to say, “hurt people, hurt our planet.” Basically, we all need to go to therapy.
People also need to reconnect with some form of spirituality (i.e., source consciousness/god/universe) to understand that we are not separate, that our seemingly insignificant individual actions have the power to both help and harm the collective. I think (hope) the COVID-19 pandemic has taught us this lesson, that we are not separate, that “the farmer in Wuhan impacts the stock broker in New York” (Steele, 2020), and the stock broker in New York impacts the factory worker in Shenzhen, whether we want to accept this truth or not. Connecting back into some type of spirituality also allows us to tap into unlimited unconditional love. And, love is really what the world needs to heal its massive wounds (well, love and therapy).
The Upper Limit Problem
Okay, let’s start by going back to our operating system: Fear 1.0. In this system, positive emotions, like the love we need to heal the world, can be a threat to survival, especially if we’ve experienced abuse, neglect or other traumas. Why? Well, because feeling good means we aren’t focused on potential danger. When we feel good, we let our guard down, we let ourselves get caught up in the joy, love or excitement of the moment and we forget about all of the horrible things that could happen to us. We may have even learned that love and abuse are paired together. This freaks out our operating system and its micromanaging supervisor, our ego. According to their programming, if we aren’t constantly scanning for danger or threats, we could be caught off guard, be attacked, and ultimately, we might not survive. So, when we start feeling positive emotions, there is a point at which our ego tells our fear-based operating system to kick back in, start worrying and start scanning for danger. Hendricks (2009) calls this our Upper Limit.
For those of you familiar with Jungian psychology, the Upper Limit is similar to the concept of a complex, which is a powerful and magnetic constellation of intrapsychic energy, often formed by severe emotional woundings. This unconscious energy is like an electromagnet, drawing similar energy to it in the forms of external experiences, belief systems and attentional focus. Complexes can be incredibly difficult to overcome and help explain why people who grow up in abusive homes tend to find abusive partners or become abusive themselves, despite their conscious desire to break the cycle (Singer, 1972).
At what point this system kicks in (i.e., where the Upper Limit is), depends on our several factors: our genes, personal history and the environment at large. If we’ve experienced abuse, neglect, other traumas, certain stressors and have a certain genetic makeup, this system is going to kick at a lower threshold than it would for those without these genes or experiences. If we experienced traumatic and stressful events at an early age and experienced them chronically, Fear 1.0 is going to kick in at an even lower threshold. We can think of it as a thermostat. Some of us have thermostats that are set higher and some have thermostats that are set lower; these settings are based upon our genes, experiences and the greater environment we grew up in (Hendricks, 2009).
In order to experience a greater level of positive emotion, we need to reset our thermostats and our expectations. In other words, we need to evolve our consciousness. If we don’t, we may have trouble hanging onto good things in our lives. For example, have you ever told yourself, “If I just won the lottery, then…[insert some iteration of ‘things will be better’ here]”? I’m going to let you in on a depressing secret: Things will not be better. 60% of lotto winners squander their winnings within two years (Hendricks, 2009). Why? Because they didn’t reset their thermostats. A happy, fulfilling life is, for the most part, an inside job, despite what our externally focused consumer culture would lead us to believe. The lottery winners needed to grow into that new money story in order to hang onto it. They needed to become the types of people who can have and hold that kind of money.
On the subject of money specifically, even if people are able to hang onto wealth, the research shows that after basic needs are met (food, clothing, shelter), money does not increase one’s level of happiness (Kahneman & Deaton, 2010). Indeed, when I’ve interviewed people who have been able to hold onto a great deal of wealth, they’ve told me that the most depressing part of receiving that much money, was when they woke up the next day to realize that their lives were no different than they were the day before. That golden ticket they thought would change everything, changed nothing. In fact, they say that the money has actually served as an accelerant, making smaller problems much larger. These are some of the most important lessons they’ve learned: Money doesn’t buy happiness and money often makes problems worse. And, because these lessons are so important and only a select few are given the opportunity to actually learn them, this select few has wanted to share these lessons with others, to spare them the pain and energy spent trying to find the pot of gold at the end of the rainbow. But, they say that when they’ve tried to impart this wisdom upon others, others are incredulous, become upset and act as if someone’s tried to take their god away. And, I suppose someone has…
This example doesn’t just apply to money. Many of us have a strange tendency to unconsciously sabotage anything good that happens in our lives. Sometimes, the sabotage comes from forces that seem completely outside of our control. For example, things are going well at work, we just closed a big deal with a new client, then on the way home, we get into a car accident. Or, things are going surprisingly well at home with our partner, then our computer crashes and we lose three months’ work. The other shoe drops, just like we expect it to. Even if the shoe never drops, even if we are able to hang onto the good things we’ve been hoping for, those elusive golden tickets, we quickly learn that they don’t have the effect of improving our lives to the degree we hoped they would, so we go in search of the next golden ticket. This is because we are focused on a happiness that is external, unstable and often material, rather than focusing our efforts internally, learning how to self-generate a happiness that’s independent of external factors.
You may have even experienced some variation of this unconscious sabotage yourself: Things feel like they are going well, you get some money in savings, and then your furnace goes out and your car breaks down. Within minutes, all of that money is gone. And you feel like the universe hates you. You feel like you just can’t hold onto money, that you just can’t hold onto good things. Well, you are sort of right about that. You can’t. Not from the space you are in. You need to become the person who has money and other, positive experiences in their life. Not only that, as we’ve mentioned, you need to understand that the positive experiences, the so-called golden tickets we find in the outside world (e.g., money, a relationship, a promotion) aren’t the key to happiness. A happy and fulfilling life truly is an inside job. This internal, becoming process takes a great deal of time, effort and patience. Unfortunately, most human beings don’t grow very much in our lifetimes. It’s estimated that, on average, we gain only about 5 consciousness points in our lifetimes, well, actually 105, but I’ll explain that in a minute (Hawkins, 2002).
I’d like to add a caveat here. Not every trial, tribulation or tragedy in our life can be accounted for by the Upper Limit Problem. Sometimes shit just happens and it isn’t our fault, as highlighted by the Bible’s Book of Job. And, in some cases, as we’ll discuss later, we may not have the ability to make major change; uncontrollable forces may be dictating much of our lives. The Upper Limit Problem just refers to a general experience of negativity in our lives, of a certain energy we tend to attract, not unlike that described by the Law of Attraction (Hicks & Hicks, 2006). The Upper Limit Problem and the Law of Attraction can be seen as general frameworks for understanding human experience; they don’t explain all of human experience.
Measuring Human Consciousness
David Hawkins (2002) developed a scale that delineates human energy vibration. Essentially, it describes where we each of us falls on this thermostat we’ve been talking about; he called it the Map of Consciousness. Hawkins states that human consciousness is much like the concept of source consciousness/god/universe: It is all things at once. All levels of consciousness are present at all times. When we have unhealed wounds, they emit low vibrational energy, which obscures the upper vibrational energy levels like a cloud or like static causing interference on a radio. In order to access the higher vibrational levels consistently, in order to tune in more precisely, we need to clear the noise; ultimately, we need to heal the pain creating the noise. This is how drugs, alcohol and psychotropic medications work: They don’t raise our consciousness/energy level per se, they medicate/numb our pain and in so doing, they clear away the lower vibrational energy noise our pain emits. As we can logically deduce, none of these substances are sustainable solutions for raising energy vibration (i.e., improving mood), despite what the pharmaceutical companies would like us to believe. Guess what does actually provide a sustainable solution for raising energy vibration by actually healing the noise-emitting pain? Yep, you guessed it, therapy (and other types of deep healing work). Otherwise known as convenient theories for me. But, really, even the research shows that therapy is an effective and sustainable way to heal the underlying pain contributing to mental health concerns (Bradley, Greene, Russ, Dutra, & Westen, 2005; Cahill, Foa, Hembree, Marshall, & Nacash, 2006; Foa, Keane, & Friedman, 2000; Harvey, Bryant, & Tarrier, 2003; Monson et al., 2006; Resick, Monson, & Chard, 2008; Resick, Nishith, Weaver, Astin, & Feuer, 2002; Resick & Schnicke, 1992, 1993).
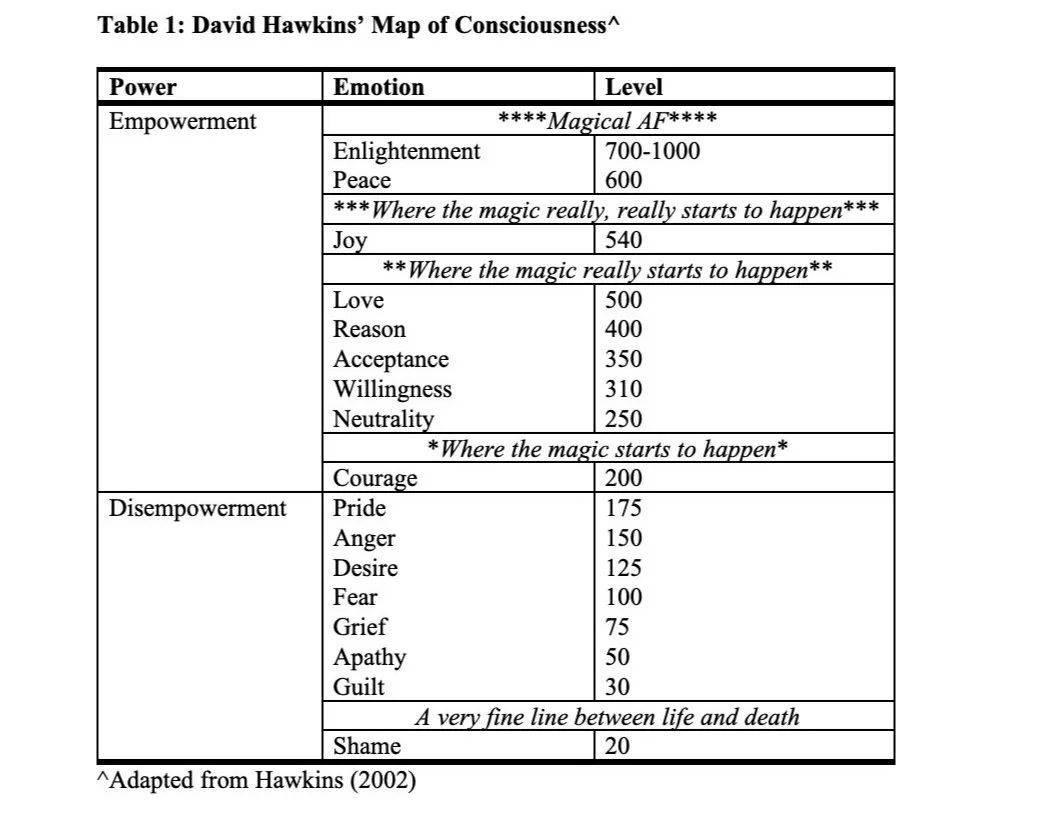
Hawkins’ (2002) consciousness scale ranges from 0-1000 with the lower numbers representing lower vibrational (lower frequency) negative emotions and the higher numbers representing higher vibrational (higher frequency) positive emotions. The scale is logarithmic, so 100 and 200 are at exponentially different levels on the scale rather than incrementally different levels on the scale (i.e., the difference between 100 and 200 isn’t 100 points, it’s 10100points). Now that I’ve demonstrated I understand math, let’s talk about the scale. The lowest level described on the scale is shame, which is given a numerical value of 20, the next is guilt with a value of 30. We’re going to talk more about shame in a little while, but for now, just remember that it is the lowest measurable point on the scale. Level 200, courage, is very important because it is the tipping point from a negative, destructive, disempowered, weak, ego- and victim-based worldview to a more positive, constructive, empowered, strength, soul- and creator-based worldview. In other words, this is where the magic starts to happen. Levels 500, love, and 540, joy, are also important because they represent turning points in energy vibrational levels, where the magic really begins to happen. The highest level described by the scale is enlightenment, with a value of 700-1000 (See Table 1). Enlightenment represents yet another turning point in energy vibrational level, albeit a rarely achieved one, but when it is achieved, those achieving it become magical AF, transcending the laws of ordinary space-time.
Courage: Level 200
The level of courage is important because is the point at which we begin to understand that we have creative power and some control over the reality we live in. Here we begin to see that things don’t just happen to us, we see that we play a role in creating our reality, including creating those events that we had previously believed were due to outside forces, coincidence or bad luck. We also develop a willingness to face our fears and overcome challenges. Our ego begins to loosen its grip on our psyches and soul steps in. We are able to cope with change and hardship without continually collapsing into despair and helplessness. Courage is the point at which we develop a drive, the energy to learn new skills, solve problems, and overcome the challenges and fears we are now willing to face. There is a newfound sense of possibility where there was once hopelessness. This is the point at which many folks decide to work with a therapist or another type of healing practitioner to do some deep, introspective work, to face their fears and traumas (Hawkins, 2002). Further, I would argue that, although someone at this level is not yet vibrating at 500, the level of unconditional love, love is often what gives someone the courage to face fears, overcome challenges, try new things, cope with change and hardship, and ultimately, begin to affect positive change in their life. So, when someone reaches the level of courage, I believe they have found a way to tap into the energy vibration of love (i.e., source consciousness) effectively enough to draw upon it for strength. We’ll talk more about the power of love throughout this article.
The tipping point at level 200, courage, is also important because this is the point at which we stop draining energy from the collective and planet, and begin to give back what we take out; that is, we break even. This happens at both an energetic and material level (e.g., consumption of resources). The more we raise our consciousness, the more we give back. One person at level 300 is able to counterbalance 90,000 people below level 200; one person at level 600 is able to counterbalance 10 million people below level 200 (see Table 2). So, if we think our individual actions don’t matter, I hope this makes it clear that they do. And, even if you don’t buy this whole consciousness scale, energy vibration thing, I want you to consider something: How do you feel after you’ve spent time with a negative person or in an unhealthy environment, where people are yelling and fighting? Do you feel joyous and energized? I doubt it. I bet you feel terrible and drained. How do you feel when you spend time with a positive person, or in a positive environment where people are kind and loving? I bet you feel uplifted, happy and restored. I rest my case.

Love: Level 500
When the magic really starts to happen is at level 500: unconditional love. At level 500, we achieve the ability to tap into source consciousness/god/universe. Even if we haven’t reached a consistent energy vibration of 500, if we are able to connect with our soul’s essence, love, using methods like meditation and dream interpretation, we can tap into source consciousness. Source consciousness is not only a source of unconditional love, it is an unlimited knowledge base (i.e., the Akashic Records).
The love we experience at this level is an expansive love that comes from within and not from external sources, from a deep connection with our heart and soul, and by extension, source consciousness. The love here provides us with compassion, understanding, and the awareness that we are all interconnected, one. This, in turn, gives us the ability to truly see others, to see them as part of us, as whole, lovable and deserving. This has the power to provide healing, deep connection, and soothe loneliness. Love is the catalyst for heroic action; it is the power that drives courage.
With love, the impossible becomes possible. This is because love gives us the courage to tackle the impossible and also, at love’s energy vibration level, we can connect to source consciousness’ unlimited knowledge base (i.e., the Akashic Records; Hawkins, 2002). Throughout history, inventors, scientists, revolutionaries and healers have used meditative and dream states to tap into source consciousness to make important discoveries, develop theories, see the future and provide healing (Moss, 2009a). You’ve probably even had some experiences with this yourself: There’s a problem that has been thwarting you for weeks (or years) and then, in the shower, doing the dishes, driving your car, falling asleep…Eureka! The solution just comes to you. This is because you’ve accidentally found a way to tap into the source consciousness knowledge base. Turns out, you can actually learn how to do this purposely, so you can tap in pretty much whenever you need an answer to a problem. How? Well, one way is through dream work. Your dreams aren’t simply random neural firings or a way for your brain to entertain itself at night, despite what modern Western culture may lead you to believe. Pretty much every other culture in the world, and even Western culture in antiquity, believe(d) that dreams serve a very useful purpose. They allow us to tap into the source consciousness knowledge base, facilitate healing and provide visions of the future (Moss, 2009a, 2009b). If I’ve piqued your curiosity and you’d like to learn more, I offer an online dream interpretation course that teaches you how to work with your dreams and access this knowledge base.
Another option for tapping into source consciousness is to begin a meditation practice. Meditation provides a basic way to momentarily clear your ego out of your mind and let source consciousness (and its infinite knowledge base) in. To begin a meditation practice, you needn’t look any further than the World Wide Web. There you will find a plethora of information about starting a meditation practice as well as some easy guided meditations to follow. As it turns out, I offer a 10-minute guided energy clearing meditation that you can download for free right here. Regular meditation also provides a number of mental and physical health benefits (e.g., improved immune functioning, lowered blood pressure, decreased cortisol levels, emotional resiliency, improved memory, better sleep), so it’s really worth giving it a shot (Bluth, Gaylord, Nguyen, Bunevicius, & Girdler, 2015; Davidson et al., 2003; Hülsheger, Feinholdt, & Nübold, 2015; Newberg, Wintering, Khalsa, Roggenkamp, & Waldman, 2010; Razon, Pickard, McCown, & Reed, 2017; Turakitwanakan, Mekseepralard, & Busarakumtragul, 2013).
The bottom line is, if more of us evolved our consciousnesses or engaged in some of these purposeful practices (e.g., dream interpretation and meditation) to tap into source consciousness, not only would more of us help humanity by raising the collective energy vibration level, we could also access the infinite knowledge base to find solutions to the major problems we are facing in our individual lives, sociopolitical systems and our natural environment. There is actually an entire group of individuals, incarnated on this planet right now, whose sole/soul mission is to raise their individual consciousness levels to 500 and above in order to raise the consciousness level of the entire collective. These individuals are called Twin Flames and you can learn more about them here.
What Love Isn’t
The world we are currently living in has an erroneous perception of love. The world confuses love with possession, dependency, and lust, which is one reason why the loss of love often turns to jealousy, anger, hate, violence and sometimes, death. In our world, love is conditional, and often transactional. If you love, honor, obey, never leave me, do what I want and make me proud, I’ll “love” you back. That’s not love, yet it’s the only love many of us ever know, from our families, lovers, friends, colleagues, bosses, mentors and leaders. The truth is, true love, unconditional love, has a lot of trouble surviving in this world, as evidenced by our sadistic affliction with killing its messengers (e.g., Jesus, Dr. Martin Luther King, Jr., John Lennon).
As we’ll learn later on, 85% of the collective favors a negative, destructive, disempowered, weak, forceful, abusive, fearful, perpetratory (yes, I made up that word), ego- and victim-based worldview (Hawkins, 2002). From this place, love, strong as it is, can be overpowered and temporarily squelched because the collective isn’t evolved enough to hold the vibration of love. Further, as the Upper Limit Problem highlights, many of us are not well equipped to tolerate high vibration emotions like love, we just aren’t evolved enough to hold those vibrations, so we unconsciously suppress and sabotage them. The good news is that love is our soul’s essence, it’s the stuff our soul is made of. And, because we all have this love within us, we all have the capacity to tap into this love, to draw upon it for power, strength, compassion, courage and infinite knowledge. The trouble is, we are often disconnected from our souls (and this love energy) and we don’t always know how to reconnect. But, fear not, there are lots of ways to reconnect, like through meditation, dream work, energy healing work and, of course, therapy. Don’t worry, I’ll give you a comprehensive list at the end.
In addition to this unhealthy societal view of love that’s based in possession, dependency and lust, there is another unhealthy view of unconditional love, of love as something without boundaries. To love someone unconditionally means, no matter what: “No matter how much they harm or hurt me, I won’t give up on them. I’ll be here, right next to them, loving them even more.” Embracing unconditional love does NOT mean becoming a doormat. Love is fierce. Love is protective. Love is love for oneself balanced with love for others. We can have love, understanding and compassion for others while setting firm boundaries with them, loving limits. We do this because we understand that to love ourselves means to keep ourselves out of harm’s way (and out of the way of harmful others). “Turn the other cheek,” does not mean, “Put up and shut up” or “Thank you, can I have another?” These phrases only allow for and perpetuate abusive behavior and are nothing more than convenient idioms for perpetrators of these behaviors. The phrase, “Turn the other cheek,” simply means that we shouldn’t seek revenge or perpetuate abusive behavior (Wikipedia-Turning…Cheek). This doesn’t mean we shouldn’t practice assertiveness and set boundaries, that we shouldn’t tell the other person to stop their abusive behavior, that we shouldn’t walk away. In fact, if we consider the self-love facet of unconditional love in this context, using a, “Thank you, can I have another?” interpretation of “Turn the other cheek,” is actually allowing someone to perpetuate abuse (abuse of you), which is exactly what, “Turn the other cheek” says NOT to do. It says not to seek revenge or perpetuate abusive behavior, which also means that you should not allow someone to perpetuate the abuse of YOU. In summary, you can love everyone on the planet, but some of those people are going to need castle walls and a moat to stay out.
Joy: Level 540
As unconditional love grows, it turns to joy. And, at this level, level 540, is when the magic really, REALLY starts to happen. Literally. At this level, spontaneous healing happens and miracles occur. Scholars suspect that this is how Jesus was able to perform miracles. His consciousness was evolved to such a high level that he had the ability to spontaneously heal the sick and perform other miracles that defied conventional wisdom. There are accounts of modern-day healers performing spontaneous healing as well (Hawkins, 2002). And, there is a great deal of evidence suggesting that sending positive energy through blessings and positive messages can promote healing and growth (Radin, 2013, 2018). Interestingly, the frequency of certain sounds (i.e., energy vibration) have been shown to be effective in healing tissue and regenerating bone. As it turns out, these sound frequencies fall in the same range as a cat’s purr, which ranges from 25-150 hertz. Cats purr not only when they are happy but also when they are under duress, injured or hungry. Scientists believe that purring serves the purpose of raising their energy vibration, which in turn facilitates physical healing and emotional soothing (Claes & Willie, 2007; Dowling, 2018; He et al., 2017; Lau et al., 2010; Omar et al., 2008; Scientific American, 2006; von Muggenthaler, 2001). This information provides a basis for understanding how an elevated consciousness level, or a higher energy vibration level, might truly produce miraculous healing effects.
As I will mention later on, when picking a therapist or other healer, it is important to find someone who has evolved their consciousness to a higher energy level, like love or joy. Unfortunately, only 4% of the population operates at level 500 (love) or above. And, only 0.4% operates at joy (540) or above, so this could be a tall order (Hawkins, 2002). But, it’s worth looking for because these folks will have special, almost magical (or actually magical) healing abilities. They might not be able to heal you in a single session like Jesus, but they will be able to find and heal things others can’t.
Enlightenment: Levels 700-1000
This brings us to the highest level on the consciousness scale: enlightenment. Enlighted consciousness is represented on the scale by the numerical values 700-1000. Enlightenment is extremely rare, with only .0000002% of the world’s population reaching level 700 or above. Spiritual greats like Jesus Christ, Lord Krishna and Mahatma Gandhi exhibited this rare, enlightened consciousness. Basically, when someone reaches this level, a religion or major spiritual movement is created around them (Hawkins, 2002). Unfortunately, many cult leaders throughout history have masqueraded as these ascended masters, only to be unveiled after their followers have thoroughly proven their undying devotion through, well, their deaths (e.g., Jim Jones).
The true ascended masters, the Enlightened Ones, don’t require their followers to prove their devotion through martyrdom. Rather, they impact all of humanity with the power of their love, grace and peace; this is how powerful their energy fields become (Hawkins, 2002). One enlightened master has the ability to counterbalance 70 million people below level 200. These individuals are so tapped into source consciousness that they develop the ability to transcend physical reality by manipulating the laws of classical physics (Radin, 2018). In other words, they become magical AF. Unbelievable as this might seem, many magical, supernatural abilities like telekinesis, telepathy, precognition, spontaneous healing and astral projection have been supported in laboratory studies and are well-accepted in the Eastern world among those engaged in advanced yogic practice; these abilities are called the Siddhis (Radin, 2013, 2018). These abilities are also described in the Bible in the context of miracles, although they are often dismissed in modern day as exaggerations or myths. So, not only is source consciousness a wellspring of unconditional love and a source of unlimited knowledge, it is the source of supernatural abilities.
Enlightenment results in a transcendence of ego consciousness and even transcendence of the physical human body. There is complete oneness with source consciousness/god/universe, such that there is no separation between the individual self and the divine source. At this level, there is little concern for the fate of the human body in an egoic sense. It is seen as merely a vehicle for navigating the Earthly plane and as a way to communicate with source consciousness/god/universe (Hawkins, 2002). This is likely why Jesus was okay with being martyred for his faith, but the rest of us view this act with horror, as the ultimate sacrifice. Unlike most of us mere mortals, Jesus fully believed that his existence transcended his physical body. Indeed, the Apostles’ Creed details the fulfillment of his belief and the Christian holiday, Easter, commemorates his enlightened ability to transcend the corporeal body: “[He] was crucified, died and was buried; He descended to the dead; on the third day He rose again; He ascended into heaven” (Apostles’ Creed, 500 AD/2012).
The death and resurrection of Jesus Christ is not the only example of this phenomenon in history. As you may recall, the Mayans were a highly advanced culture, with a societal structure, belief systems and technological advances that rivaled those of the ancient Egyptians (Shneiderman, Sanders, & March, 2017). But they vanished without a trace. Some hypothesize that they didn’t simply vanish. Some believe that enlightenment and its resultant superhuman abilities may explain the fate of the Mayans: The ancient Mayans were so spiritually advanced and their consciousnesses so evolved, that they were able to transcend their physical bodies and leave the Earthly plane without a trace 💥 (Redfield, 1993).
Shame, Shame Know Your Name: Level 20
I want to backtrack to talk about shame, which is the emotion associated with the lowest level on the consciousness scale. I hate to talk about emotions as good, bad, right or wrong, but I feel like this is an exception. Shame is an incredibly dangerous emotion. It is usually something that is given to us by another person who was experiencing their own shame, which they found intolerable, so they projected it onto an external source (us) in order to deal with it there, in a more removed and less emotionally charged manner (less emotionally charged for them anyway). Shame is marked by the feeling of complete humiliation and the behavioral urges to hide and disconnect from others. When we feel this emotion, we feel less than human, completely unworthy of love and belonging. Acts that the culture considers shameful can result in ostracism; losing your place in society. Earlier in our evolution, banishment most assuredly meant death. Even today, it is nearly impossible to survive without the support of at least a few others. For these reasons, shame remains tantamount to death. And, it is when people are feeling an enveloping level of shame, that they will actively attempt to die by suicide, will make passive attempts at suicide (e.g., driving recklessly, not taking necessary medications, abusing drugs or alcohol), will have avoidable accidents, or will become serial killers. This is because, in the throes of shame, the line between life and death has essentially evaporated for them. They take the shame-inducing cruelty that was inflicted upon them by others and they project it inwardly to create potentially deadly self-loathing, or project it outwardly, making others feel the shame they can’t bear to feel themselves, sometimes with sadistic results, as seen in serial killings. Shame is like a disease, transmitted from human to human through the defense mechanism of projection.
When people do harmful things to others because of their own shame and woundings (i.e., hurt people, hurt people), they are often haunted more by these events than by the awful things that happened to them (unless, of course, they are sociopaths). They can find the compassion to forgive their perpetrators but they can’t find the compassion to forgive themselves. They have trouble seeing themselves as anything other than terrible, soulless monsters. They fail to recognize that their regrettable actions didn’t occur in a vacuum, that there were likely survival-based reasons for those actions, and that the shame, regret and remorse they currently feel indicate that they do still actually have a soul. In some cases, they experience their actions as so horrific that they go on to develop what’s called perpetration-induced trauma, a type of posttraumatic stress disorder (PTSD) that results from perpetrating harmful acts upon others, animals or the environment.
We live in a world that has no shortage of shame-inducing events, with sexual abuse as one of the nastiest culprits, triggering its victims into the depths of a shame hell, decades after it occurs. And, the use of shame to punish children and adults is rampant, dangerous, and cruel, found in our individual family systems, educational institutions and in our sociopolitical structure (e.g., the criminal “justice” system; Hawkins, 2002). We use shame to cut young boys off from their tenderness, vulnerability and empathy, and to cut girls off from their anger, power and ambition. These processes have disastrous personal and cultural consequences (e.g., substance abuse, heart disease, depression, antisocial behavior and relational problems in men and dependency, anxiety, depression, victimization and powerlessness in women).
Shame as an Ineffectual Tool for Social Change
Our culture also uses shame combined with forceful power to address social problems at the symptom level rather than at the root. If this actually worked, it might be worth examining further. But it doesn’t. Not even close. For example, drunk driving is a large societal problem that we’ve tried to solve through force and shame induction, using the power of the criminal justice system. But, drunk driving isn’t the actual problem. Drunk driving is usually a symptom of a larger, substance use problem. Substance use isn’t even the actual problem. Substance use is actually a solution to a problem (Klott, 2011), a mental health problem, such as depression, anxiety or PTSD. That mental health problem is the result of yet another problem still: unhealed emotional wounds that come from abuse, neglect and other traumas, from soul injuries. The substance use provides a temporary solution by numbing and distracting from the pain and other symptoms that arise from the soul injury. When we understand the complexity of the problem, we understand that our societal “solution” of imposing criminal consequences for drunk driving, punishes, rather than helps people with traumatic woundings, serving as an indirect form of victim blaming. (And, yes, I know that the “justice” system mandates some type of substance use education for drunk driving “offenders,” but respectfully, those courses are basically useless. We need to do better.)
With this example, we can see how we try to force social change by using shame and power (e.g., political, legal) to fix the symptom of a problem (e.g., drunk driving) when we should be trying to promote change by using compassion and empowerment to heal the root of the problem (e.g., abuse, neglect or other traumas; Hawkins, 2002). Convicting someone of a crime, imposing astronomical fines, revoking mobility privileges, imprisoning them, and requiring special license plates that all but say, “I’m a drunk,” only serve to make a large, shame-filled problem much worse for people. Not only that, these are completely ineffectual solutions.
What might actually solve the problem is to devote more money to mental healthcare in this country, good mental healthcare. Promoting good mental healthcare means graduating more highly trained practitioners and providing high-quality continuing education, both of which currently come at a major cost to the practitioner. These practitioners are already poorly compensated for the work they do, which is very difficult, emotionally deleterious and sometimes, even dangerous work. The high training costs, the great emotional burden of the work itself, the significant amount of recovery time and self-care required to perform the work competently (which are currently impossible to achieve due to the significant demands of the job and low rates of pay) and the relatively low compensation rates, lead highly trained practitioners to leave the field due to burnout, moral injury and financial instability, and de-incentivize potential practitioners from ever entering it to begin with. You can read more about that here. If we want to fix the mental health crisis in America, we can start by doing a much better job supporting mental health providers, both emotionally and financially. Fun fact: Did you know that we pay commercial truck drivers more than we pay most of our highly educated therapists? (PayScale). This data point highlights the values system in our country: We value the people who transport our consumer goods across the country more than we value the people who care for our mental health; and by extension, we value our consumer goods more than we value our mental health.
Another helpful solution would be to develop additional public service movements designed to destigmatize mental health problems, so more people would feel comfortable, rather than ashamed, to admit they have a problem and subsequently receive help. For the issue of drunk driving specifically, what might actually help, is rather than investing money in law enforcement to arrest drunk drivers, investing this money in alternative transportation resources, not only in public transportation but in subsidization of cab and car services, especially for those in rural communities.
So, rather than utilizing a shame- and power-based societal response that says, “If you drink and drive, you are a criminal. Go sit in jail and think about what you’ve done!” We could utilize a compassion- and empowerment-based societal response that says, “We know you are struggling with some really painful issues right now, but you still can’t drink and drive. We’re going to provide you with the resources you need to heal as well as some safe transportation alternatives.” What a revolution that would be.
If you’re wondering where all of this money might come from given the multitrillion-dollar budget deficit our government is currently running at, I have an idea: Maybe stop investing so much money in the GD defense budget. Do we really need to possess the ability to blow up the Earth 4 times? Like, is that even necessary? It’s just one gigantic, and very dangerous, pissing contest. And, proof positive that many of us haven’t evolved beyond our time on the playground. And, maybe, if some of us didn’t act like such power-hungry, land-snatching assholes, we wouldn’t need to worry about the threat of nuclear war. Guess what could reduce that threat? Healing our wounds and evolving our collective consciousness by getting some mental health treatment. But, then again, defense contracting is big business and eliminating the threat of warfare would cut into profit margins, as well as disrupt the corporate-congressional circle jerk that’s maintaining those profit margins. So…what to do? What to do?
Another great idea would be for the government to stop giving our tax dollars to the fossil fuel companies, who are destroying our planet, and start giving our tax dollars to mental health services and organizations, who are actually improving the state of humanity, and by extension, the planet itself. In 2019, the U.S. government’s fossil fuel subsidies totaled around 555 billion dollars (Timperley, 2021). In contrast, the government’s 2019 budget allocated only 10.6 billion dollars to mental health and substance use research, treatment, and training. In other words, the government decided that the tax payers’ money would be better spent helping the oil and gas industry become more profitable, rather than spent creating services to help suffering Americans and ultimately, improving the state of humanity (American Psychiatric Association, 2019). This is another data point that illustrates what we value in this country, and it’s clearly not our mental health.
Further, the fossil fuel industry is a huge part of the reason why we are experiencing catastrophic climate change. Reports have begun emerging that the fossil fuel industry has known for decades that it is contributing to “dramatic environmental effects.” Indeed, their own scientists documented the widespread deleterious effects of fossil fuel emissions pollution as early as 1951—70 years ago! But, the fossil fuel industry 1) has not curtailed its behavior and 2) in fact, has actually hidden this data from the public, going so far as to actively repudiate the scientific evidence substantiating climate change, because admitting this would not only mean incrimination, it would mean loss of revenue (Jones, 1958; McGreal, 2021; Supran; Supran & Oreskes, 2017, 2020). It sounds a lot like what happened with the tobacco industry a few years back. And, just because this is the way things areright now and have been for some time, doesn’t mean that this is the way things need to continue. Each of you has the power to change this. If you are mad as hell about this, like I am, at the end of this article, I provide a list of environmental organizations you can join, where you can sign petitions, create your own petitions, donate money and send letters to Congress, demanding change, accountability and restitution. You can also view an expert’s presentation on the fossil fuel industry’s climate change coverup here.
Oh, and before I forget, let me address the ever-popular counterargument that the fossil fuel industry likes to use: But, we create jobs! Yes, you do create jobs. But at what cost? The tobacco industry also created jobs but we had to get past that argument and phase those jobs out. Turns out, clean energy creates jobs too. Maybe, we should give that a try. We could even allocate some funding to retrain fossil fuel industry workers to work in clean energy, or we could help them find new jobs. I’m pretty sure there’s a solution here that doesn’t involve continuing to destroy the planet so nothing has to change. And, let’s be honest, this argument isn’t really about the fossil fuel industry workers, it’s about profit margins and stock portfolios. But, I digress. What were we talking about? Oh, yes, shame. Never mind. We are right on topic.
What to do About Shame
Alright, so shame is clearly a big problem. What can we do about it? I’m going to give you some methods at the end that will help raise your energy vibration in general. These methods will, by extension, also help with shame. But I want to take a moment now to address how to heal shame specifically. The most important fact to understand about shame is that it dies when it’s exposed to light. So, the best way to heal shame is to confess your shameful secrets, to bring them into the light. There are many ways to do this. One relatively safe and easy way to bring them to light is by writing them down in a secret place where no one will find them. When you are done, burn or delete them. After you’ve tried this exercise, decide if you’d like to take it a step further by actually confessing your shameful secrets to a person. This will serve several purposes, 1) like writing them down, a verbal confession will bring the shameful secrets to light, effectively burning them away, 2) if the person responds compassionately, this will provide you with evidence that your shameful secrets don’t make you a terrible person who is deserving of humiliation and scorn, also helping to burn the shame away, and, 3) shame compels us to hide and disconnect from others, resulting in self-imposed ostracism, so confessing shameful secrets brings you out of hiding, reconnects you with others and ameliorates ostracism.
Before you take this step, I caution you to only tell your secrets to a trusted person, someone who has a history of being loving, nonjudgmental and compassionate. If you tell someone you don’t trust completely, who can be unloving, judgmental or lack compassion, you run the risk of adding additional shame to your shame pile, rather than reducing it. Not good for healing. If you’ve done something illegal, it might be worth telling someone who is bound by confidentiality, like a therapist, lawyer or priest. Generally speaking, therapy can be a good place to confess your shameful secrets. Many therapists are loving and nonjudgmental, and frankly, they’ve pretty much heard it all. So, it is unlikely that what you say will shock them or produce a judgmental response. Of course, there are no guarantees, but generally speaking, therapists are one of the safer bets for shame confessions.
Where Do You Fall on the Consciousness Scale?
I bet you are wondering how you can find out where you fall on the consciousness scale, wondering if you are a secretly an ascended master who will establish the world’s next major religion. Unfortunately, I don’t have a great answer for you. The consciousness scale was creating using a muscle testing technique, which came out of the field of kinesiology. Researchers discovered that muscles go weak when exposed to harmful physical or mental stimuli (e.g., artificial sweetener, cruel words) and demonstrate strength when exposed to beneficial physical or mental stimuli (e.g., nutritious foods, kind words). Although relatively foreign to Western medicine, this technique is widely used in holistic medicine. You may have even heard of the use of this muscle testing technique to diagnose certain allergies (Hawkins, 2002). I’ve never used this muscle testing technique to measure consciousness levels, so I don’t feel confident in attempting to instruct you on how to use it. Instead, I’d recommend taking a look at the descriptions of the different levels on the consciousness scale, using the link here (Huseyin, 2016). Next, consider how you typically respond when under stress, and then determine which emotion description (e.g., pride, shame, courage, love) most accurately describes your response. Most of us can hold it together when things are going well, but when stress is applied, our masks fall and our true character is revealed, so this exercise should give you a fairly decent estimate of where your consciousness level lies.
When making your guestimates, keep in mind the base rates for the levels on the scale. As we’ll learn in a minute, 85% of the population scores below 200; 4% scores above 500; 0.4% scores above 540 and .0000002% scores above 700. In other words, I doubt anyone reading this has reached 700, enlightenment (including the person writing this), so you can go ahead and rule that option out. Scores above 500 are also pretty unlikely but not impossible. Because you are reading an article on the evolution of consciousness, that tells me you have at least some interest in self-improvement and may have done some work on this, so you are more likely than the other 85% of the population to score above 200, but you can take a look at the scale descriptions and decide for yourself. And, if you do score above 200, please don’t use that as a free pass to stop growing as a human. As we’ve discussed and will continue to discuss, we all have work to do, even the ascended masters.
How Are We Doing as a Whole? Humanity’s Consciousness Score
Now that you’ve figured out where you fall on the consciousness scale, let’s discuss how human beings are doing as a whole. In the mid-1980s, the energy vibration of humanity as a whole was estimated at 207 (Hawkins, 2002). (It might be higher now, but I wasn’t able to track down that exact statistic.) This is actually good news considering that the level had remained at a stagnant 190 for centuries prior to the mid-1980s. I say this is good news because it means humanity as a whole has crossed over the tipping point, to courage, which means that we may actually have a prayer of unfucking the Earth and our social systems before our home planet becomes uninhabitable.
However, before we get too excited about this and think that our work here is done, let me point out a couple pieces of disconcerting information. First piece of disconcerting information: Our beloved friend, Koko the Gorilla, had an estimated energy vibration of 250. For you math wizards out there, this means that a primate outscored her supposedly more evolved human counterparts by 1043. Second piece of disconcerting information: The number 207, humanity’s average, is actually misleading. Let’s talk about the statistical distribution of that number. Averages are tricky little buggers, and are easily influenced by what’s called a skewed distribution. Statistics assume that when a scale ranges from 0-1000, the scores are distributed in a bell shape, with the bulk of the scores falling in the middle, representing the average of the population. So, when we hear the number 207, we may be inclined to think, “Oh, great; most of the population is functioning at the courage level.” No such luck. Averages can pulled up or down by that skewed distribution I just mentioned. So, rather than falling in that perfect, bell-shaped curve, the scores fall more heavily on one end or another, or both. Humanity’s consciousness has a skewed distribution problem: 85% of the population functions below 200, and 15% functions above 200, with 4% functioning above 500. That 4% of the population scores so high on the logarithmic consciousness scale that they pull the average up for the entire population, making it appear as if humans are doing pretty well as individuals (Hawkins, 2002). We aren’t. We have some serious work to do. But, don’t lose hope. We’ll discuss some interesting supernatural, statistical, behavioral and quantum physics’ phenomena that could help humanity speed up this process. And, we’ll also discuss what you can do individually to help with the process.
What do the Law of Diffusion of Innovations, Morphic Resonance, String Theory (M-Theory), Quantum Entanglement and Synchronicity Have in Common? Source Consciousness.
The Law of Diffusion of Innovations, Morphic Resonance, String Theory (M-theory), quantum entanglement and synchronicity all help explain how certain information spreads in an unusual, nonlinear and sometimes, instantaneous manner. With the exception of String Theory (M-theory)*, I’d even go so far as to hypothesize that they are simply different terms describing the same underlying phenomenon: extrasensory perception arising from source consciousness (also called group consciousness in some circles). What? Yeah. ESP. Remember how we discussed earlier that individuals with an enlightened consciousness were so tapped into source consciousness that they developed supernatural abilities? Well, it appears that all of us are able to tap into source consciousness to some degree, which allows all of us to utilize some of these abilities at various times to varying degrees.
*(As discussed below, String Theory postulates additional dimensions, like a source consciousness dimension, that could enable extrasensory perception, but it doesn’t speculate about extrasensory perception itself.)
Physicist Max Planck (1931) believed that consciousness (analogous to the concept of source consciousness that we’ve been discussing), including our individual consciousness, underlies everything—everything—in the known universe, and is therefore capable of interacting with everything in the known universe. In other words, a change in the consciousness of someone on Earth can cause a change in the consciousness (or even the physical structure) of a rock on Mars, strange as that may sound. Indeed, as physics has advanced, concepts such as quantum entanglement and String Theory (M-theory) have been developed, suggesting that the universe is interconnected, interactive and multidimensional. Research into these theories has provided an empirically supported basis for the concept of source consciousness at both the macro and subatomic levels (Greene, 2004; Moss, 2009a; Radin, 2018).
We could think of source consciousness as another dimension existing outside of the three dimensions we currently experience on Earth; this would be a dimension that we cannot see because we are currently trapped by the physical limitations of our three dimensions. This conceptualization may seem difficult to grasp, but it’s not as difficult when we consider what our three-dimensional world, which we know fully exists, would look like from the perspective of someone who lives in two dimensions (e.g., a flat person on a flat piece of paper). That person would only be able to experience a three-dimensional existence in flat slices (planes) of that 3rd dimension (Sagan, 1980). (If you’d like further explanation, I’d recommend watching Carl Sagan’s Cosmos episode, “The Edge of Forever,” discussing the Tesseract and Flatlanders.) Indeed, physicists postulate that the universe is made up of many more dimensions than the three we are capable of experiencing as humans on Earth, as elucidated by String Theory (M-theory). These extra dimensions are made up of subatomic particles, called strings, and these strings have different energy vibrations (Greene, 2004), just like human consciousness has different energy vibrations. Taking these theories together, if source consciousness does exist in another dimension, we would be able to access it (and it could access us) when we raise our consciousness to the vibrational level of the strings in source consciousness’ particular dimension (i.e., 500, unconditional love and above), and could subsequently unlock a variety of superhuman abilities, unconditional love and an unlimited knowledge base.
This idea is even more plausible when we consider how other energy frequencies work, like the classes of electromagnetic radiation within the electromagnetic spectrum; these different classes represent different frequencies of energy. Within the electromagnetic spectrum, we can only detect with our physical senses, those energy frequencies within the class of visible light; we are only able to see the sights (i.e., energy frequencies) our eyes can detect. However, many other types of energy frequencies exist, such as radio waves, X-rays, gamma rays, infrared light, and ultraviolet light. Our five physical senses cannot detect these, but they most assuredly do exist. We know these exist because we have invented machines that are able to detect these, are able to tune into these energy frequencies by using a corresponding frequency, and can utilize these energy frequencies to communicate information across space-time (e.g., radio waves are a form of mechanical telepathy), and detect what our ordinary senses cannot (e.g., X-rays can see broken bones through opaque skin and muscle). If we were able to tune our bodies to different frequencies (e.g., that of source consciousness), just like we can these machines, we could ostensibly unlock the special powers of these frequencies, in the same way we can tune an X-ray machine to tap into the special powers of the X-ray energy frequency.
Relevant to our current discussion are the source consciousness supernatural abilities of telepathy (i.e., the ability to communicate without known sensory organs, through source consciousness) and telekinesis (i.e., the ability to manipulate physical matter with one’s mind/consciousness); these abilities demonstrate source consciousness at the macro level. At the subatomic level, the abilities to communicate telepathically and affect physical change across space and time telekinetically are what Einstein referred to as, “spooky action at a distance,” and later physicists labeled, quantum entanglement (Greene, 2004; Wikipedia-Quantum Enganglement). Under quantum entanglement, a change in the state of one entangled particle will produce a parallel change in its entangled counterpart, unbound by space-time and conventional communication methods, such that an entangled particle on Earth will change at the same time and in the same way as its entangled counterpart on Mars. The concept of quantum entanglement may very well substantiate the subatomic underpinnings of macro-level phenomena like telepathy and telekinesis.
Psychiatrist Carl Jung and physicist Wolfgang Pauli collaborated extensively on the phenomenon of source consciousness, and how it manifests in the physical world as mystical communication (i.e., telepathy) and changes to physical matter (i.e., telekinesis). They, like Planck (1931), believed that consciousness was the base “substance” of everything in the known universe and that a phenomenon they called, synchronicity, provided evidence for this omnipresent, spiritual (source) consciousness in the physical world (Cambray, 2009). In other words, synchronicity provided evidence of this additional dimension of source consciousness “breaking through” into our three-dimensional reality. Synchronicity is defined as “a unique moment ‘falling together in time,’” (Cambray, 2009, p. xi), where inner and outer worlds meet; and meaning is the component that holds them together. “That which is above, is like that which is below” (Trismegistus, p. 12). Synchronicity can be thought of as the intersection of the unseen, spiritual world (i.e., source consciousness) with the seen, physical world we currently live in. And, as specified by Jung and Pauli, meaning needs to be involved; there needs to be a relevance, an intention, an emotional charge, a soul-aligned connection to source consciousness in order to bring synchronicity into the physical world. Synchronicities are often what many of us refer to as signs; those weird, supposedly coincidental communications that feel too meaningful to simply be dismissed as mere coincidence (i.e., a form of telepathic communication). Miraculous events also fall into the synchronicity category—help that arrives just when we need it, the new opportunity that seems to be an answer to our prayers, the unexplainable recovery from a serious illness (i.e., forms of telekinesis). These experiences all leave us with a strange feeling, they stop us in our tracks and make us question the conventional nature of reality; or as Jung put it, they give us the sense that there’s been a “rupture in time,” as if the fabric of the known universe has opened and let something otherworldly in (Moss, 2015). And, indeed, this may be what is happening: Another dimension is breaking through into our three-dimensional reality.
The concept of source consciousness has also been studied in the business world and in the behavioral and biological sciences, but not many are calling it this, especially not in the business world. In business, there’s a concept called, the Law of Diffusion of Innovations. It states that when a product or service achieves a 15-18% market buy-in rate, the product or service “takes off” at an exponential rate and then achieves market-wide success (Rogers, 1962; Sinek, 2009). In other words, it becomes popular, a household name. The same is true of new ideas. Of course, those in the marketing sector have been keen to deconstruct and harness this phenomenon, in order to artificially induce mass market product adoption. In his groundbreaking book, Start with Why, Simon Sinek (2009) postulates that ideas and products take off faster when the product or idea has a clearly articulated why that aligns with the values of the consumers. He says, “People don’t buy what you do, they buy why you do it” (p. 41). This is similar to the most essential component of synchronicity: meaning. There needs to be meaningful, soul-aligned connection with source consciousness in order to spur the phenomenon of synchronicity. And, there needs to be a meaningful, soul-aligned why in marketing to more quickly spur mass market adoption of a product or service under the Law of Diffusion of Innovations. Despite this deep understanding of the Law of Diffusion of Innovations, no one seems to have recognized and acknowledged that there is a larger force underlying the phenomenon: source consciousness. That’s probably because concepts such as source consciousness, although gaining some traction in quantum physics and parapsychology, are still regarded as pseudoscientific hocus pocus across much of the scientific community and are all but dismissed by the rational, Western business world.
The behavioral and biological sciences have also documented group consciousness in their research and theories, though the majority of scientists do not use this term nor do they acknowledge that supernatural phenomena like group consciousness or extrasensory perception exist, which is unfortunate, because it impedes scientific advancement and interdisciplinary collaboration. A pioneer, by the name of Rupert Sheldrake is challenging conventional wisdom in the behavioral and biological sciences. He has devoted much of his career to studying a phenomenon he calls, Morphic Resonance. Morphic Resonance describes how certain behaviors “build up” in a species over time. When the behaviors reach a critical mass (i.e., a high enough level of adoption among members of the species), this behavioral information is automatically transmitted throughout the species, seemingly unbound by space and time, and without the use of known sensory organs, such that a member of the species on one side of planet will adopt the same behaviors as their counterparts on another side of the planet. In effect, it seems that members of the species are able to transmit and absorb this new information telepathically via group (source) consciousness. As unbelievable as this may sound, Morphic Resonance, telepathy and group consciousness have all been supported in laboratory and observational studies (Radin, 2018; Sheldrake; Talbot, 1988).
In case you missed it the first few times I brought it up, let me state it very clearly now: Supernatural phenomena have been empirically studied and supported by scientists, using rigorous methodology (Radin, 2013, 2018). Does this seem unbelievable? Are you wondering why you don’t know about this yet? I’ll tell you why: Because research findings on spooky phenomena such as group consciousness and telepathy are usually dismissed, labeled pseudoscience and essentially hidden from the public by the scientific community. Why? Because, just like the rest of society, the scientific community contains the full spectrum of human consciousness, including those with evolved consciousnesses and those with less evolved consciousnesses. And, like the rest of society, the preponderance of the scientific community is made up of those with consciousness levels below 200, which means they are driven primarily by their egos and fear. These individuals have egos that can’t bear the possibility that what they’ve believed their entire lives, what they have based their entire life’s work upon, could be completely wrong, resulting in their personal irrelevance, a fate worse than death in the scientific community. So, they enlist one of their trusted defense mechanisms (e.g., denial, repression) to make sure that these new, “preposterous” research findings never reach the masses (Radin, 2018), thus ensuring their continued relevance and thwarting scientific advancement in the process. Fear 1.0 strikes again.
Okay, so how are the concepts of source consciousness, the Law of Diffusion of Innovations and Morphic Resonance relevant for evolving human consciousness and ultimately saving our species from complete and total destruction? Good question. These concepts suggest that we don’t need to evolve the minds of everyone on the planet, we just need to evolve the minds of a critical mass. When that happens, the evolution of consciousness and its corresponding humanity-saving ideals will take off; they will be spread via source consciousness; they will become popular, household names; consciousness evolution will be all the rage. And, according to Hawkins’ (2002) consciousness data and the tipping point identified by the Law of Diffusion of Innovations (Rogers, 1962; Sinek, 2009), we’re already in the home stretch: 15% of the population has reached the consciousness tipping point of courage, at which point our energy flips from depleting the collective to replenishing the collective. This corresponds to the Law of Diffusion of Innovations, which states that a 15-18% mass market adoption rate is the required tipping point for an idea to take off. When we consider these data, we can see that if just a few more of us took up the torch of consciousness evolution, we could use it to light the way for the rest, saving humanity in the process. Alternatively, that critical few of us could simply choose to watch the torch drop to the ground, hoping someone else will pick it up and do the work for us, while we simply bear witness to the world burning down around us. Which option will you choose: action or apathy?
How We Can Evolve Our Consciousness
So, how do we move up the consciousness scale? How do we ultimately change the world? Do your GD work! Option 1: Go to therapy. Or, do another type of healing work (e.g., energy healing) that directly addresses your wounds. Experiencing abuse, neglect, other traumas and stressors lowers our energy vibration. This is because these events/experiences cause us to feel lower vibration emotions like shame, guilt, fear, apathy, grief and anger, which in turn emit noise that drowns out the upper level vibrations, ultimately keeping us at a lower vibrational level. If we aren’t able to address and process these events right away (and most of us aren’t because of our circumstances), these events stick with us, causing us to re-experience the negative emotions we originally felt at the time of the event as well as re-experience the memories of the event itself. Over time, these events begin to shape how we view ourselves, the world around us (including other people) and our future; they change our entire belief system. Aaron Beck called this the negative cognitive triad (Beck, Rush, Shaw, & Emery, 1987) and he believed it played a central role in the development and maintenance of depressive disorders. He believed that by changing our beliefs about ourselves, others, the world around us and our future, we could change how we felt and ultimately, improve our quality of life. Thus, these became the central tenets of his Cognitive Therapy (and later Cognitive Behavioral Therapy). Others have expanded his theory to include other disorders such as PTSD, using his conceptualization in treatment to directly address the formative role of traumatic experiences on how we view ourselves, others and the world around us (Resick et al., 2008).
To summarize, when bad things happen to us, they change what we believe, how we feel and how we perceive and experience our reality. A hypothesized universal law, called the Law of Attraction, asserts that what we believe and how we feel (our overall energy vibration) governs our perceptions of the world and even our literal physical reality. It says that we see (perceive) things and attract experiences we believe and feel we’ll see and attract, and we do so telekinetically and usually unconsciously. As discussed, Cognitive Behavioral Therapy’s central tenets are that our negative beliefs affect how we see (perceive) ourselves, others, the world, and our future, and by changing these beliefs, we have the power to change how we feel, what we perceive and how we experience life. Indeed, the research has shown that by changing our negative beliefs through Cognitive Behavioral Therapy, we can relieve symptoms of mental health disorders and improve our quality of life; that is, changing our beliefs changes our reality (DeRubeis et al., 2005; Hofmann, Moscovitch, Kim, & Taylor, 2004). As you can see, the Law of Attraction and Cognitive Behavioral Therapy operate from very similar theoretical bases, though no one seems to have tied them together before, probably because very few people in the field of psychology would ever subscribe to a theory as esoteric as the Law of Attraction, or endorse telekinesis. But, I would, and I propose that the Law of Attraction (and by extension, telekinesis) is the mechanism of action through which Cognitive Behavioral Therapy works. In other words, the reason why changing beliefs through Cognitive Behavioral Therapy is an effective method for changing the experience of reality is because the Law of Attraction exists as a type of universal law, governing our experiences.
In addition to producing a global effect of negativity, impacting our entire belief system and changing our realities, negative events and experiences can lead to acute reactions when we experience a triggering event (e.g., thought, emotion, smell, sound, situation, person); that is, an event or cue that reminds of us of the original painful event. When we experience a triggering event, we are effectively pulled back down into that original painful experience, whether we are consciously aware of this or not. It’s almost as if we leave our current reality behind and momentarily return to the old reality (and in the case of flashbacks, the legitimacy of this shift in realities feels undeniable). We are pulled back into the same emotions we felt at the time of the traumatic event (e.g., shame, fear, guilt), the physiological sensations, and also, the memories, if we have access to them. Although we may develop elaborate defense mechanisms (e.g., projection, reaction formation, denial, dissociation, repression, intellectualization, distraction, numbing, deflection, people pleasing) to protect ourselves from fully remembering and re-experiencing these painful events in conscious awareness, the wounds remain, albeit well-hidden and protected.
Emotional pain works much like physical pain: It doesn’t go away, unless properly acknowledged and healed at the source. That is, it doesn’t simply stay inside us, safely walled off in a lead container. We project it out onto the world unconsciously and we interact with it there. We do this because we cannot tolerate interacting with our pain internally. It feels like too much to bear. Why do you think the world looks the way it does, why we have war, hatred, abuse, neglect, genocide, racism, misogyny, oppression, rape, murder, sex trafficking, forced labor, dictatorships, pollution, deforestation, mass extinction, climate change, overdevelopment, consumerism, martyrdom, codependency and victimhood? These are examples of us projecting our unhealed wounds onto external sources. We are operating in survival mode, where self-interest is paramount and the energy is destructive (to others and ourselves). Even a prosocial behavior like helping others can be harmful when it is projected from a place of wounding, because from this place, it’s not about helping the other person, it’s about trying to help ourselves. This “helping” behavior can turn into caretaking, effectively robbing the other person of their autonomy, enabling bad behavior and still never getting us what we are seeking—to be taken care of. The behaviors I’ve described above are all the result of our operating system, Fear 1.0 and its defense mechanisms. These destructive behaviors are the reasons why we need to evolve that operating system, why we need to have an evolution of consciousness.
Despite our best defense mechanisms, our unhealed pain is always impacting our lives and the lives of those around us, regardless of whether we see this or not, and regardless of whether we try our damnedest to prevent this from happening. Sheer willpower and awareness do help, but they aren’t very accurate strategies. This is because, as you may recall, most information processing happens outside of conscious awareness. So, we can make a conscious effort to become aware of our wounds and the impact they have, and we can try to make sure they don’t have an impact, but at the end of the day, we don’t have very much control over them, because we simply don’t have the ability to consciously process all of that information. The real solution, the way we can regain control, is to heal the pain, so it’s not running under the surface, being projected onto the world, consciously or unconsciously.
Carl Jung said that we have an ethical responsibility to become aware of our wounds and heal them so we aren’t projecting them onto the world, harming others and also, so we aren’t a target for perpetration, because having unhealed wounds makes us vulnerable to exploitation by others (Aron, 2016). He said that when we don’t do our work, the collective has to carry us. His assertions are in line with our earlier discussion on the tipping point of the consciousness scale. When our energy vibration dips below 200, below the courage level, we are operating in survival mode and draining energy from the collective. When our vibration is at 200, we maintain equilibrium, neither supplying nor draining the collective. And, when our energy moves above 200, we are adding to the healing energy of the collective, helping to uplift others.
Now, this doesn’t mean that when we hit 200, we are cool and our work here is done. Level 200 is just an average of our overall energy vibration, sometimes our energy might be at a higher level and sometimes it might be at lower level. This means that we can still dip down below 200 and enter a place where we harm others or where others can harm us. Even if we’ve managed to move ourselves up into enlightenment, we can still dip back down into the lower levels because of situational influences. Grief, for example, can pull us back down to a 75 temporarily (Hawkins, 2002). Experiencing a trauma trigger in our environment can pull us down to a 100 (fear) and potentially even lower, into guilt (30) and shame (20). And, we can stay rooted there for some time, especially if we aren’t consciously aware of what has occurred. So, this is why it’s imperative that we heal our wounds. The more we heal, the higher our overall energy vibration and the lower our chances of being triggered by trauma (because there’s nothing left to trigger us) and subsequently dropping back into those incredibly low energy vibrations where we can fall into perpetration and victimhood.
Healing our wounds doesn’t mean that we will no longer experience lower vibration emotions. We actually need to be able to experience the full range of human emotion, no matter how low the vibration. Emotions are useful. Their job is to give us information about our environment, just like our five physical senses give us information about our environment. In a perfect world, one in which we haven’t been traumatized, this emotion-based informational system works well. So, when we feel fear, we know danger is nearby; when we feel anger, we know we have been violated; when we feel joy, we know something is making our soul happy. And, when the environmental stimulus is no longer present, the emotion dissipates relatively quickly. When we have been wounded, however, the system does not work like this. When we have been wounded, the emotion we felt at the time of the wounding and all aspects of that experience are stored deep within us, like in a pocket or a root. Later, when we experience something closely resembling that wounding experience or even a small aspect of it (e.g., smell, sound, memory flash), that entire pocket or root becomes activated. When the new experience has passed, the emotion doesn’t dissipate like it is designed to, because it has become grounded or rooted in something much deeper. This is when we can become stuck in a lower vibrational state. When we heal the wound, we still feel the full range of emotions, but, because we’ve healed the place the emotion was rooted, the emotions are able to dissipate as they are designed to, and we don’t spend a lot of time rooted in a lower vibrational state.
The trauma that is stored in the root or pocket doesn’t just have the ability to root us in lower vibrational emotions when activated by something in the present, it also serves as a generator for negative emotions, memories, thoughts and experiences, spontaneously producing these, even when outside circumstances are relatively benign. We can do our best to catch these when they arise, and attempt to move ourselves into higher vibrational energy and positive thought reframes, but this requires constant vigilance and because of the automatic and unconscious nature of this generator (and our inability to consciously process all of the information we take in), it is impossible to catch and positively reframe everything it produces. The more reliable, effective and sustainable approach is to heal the underlying trauma at the roots, so it can no longer serve as a generator for negative emotions, memories, thoughts and experiences. In conclusion, we need to do the hard work.
Option 2 for consciousness evolution: Read some self-help books, work with various healers (e.g., Reiki practitioners, acupuncturists, mediums), do yoga, listen to podcasts, meditate, journal…basically choose your own personal-growth adventure. These options will help raise energy vibration, and I think they are an essential part of any personal growth and healing journey, but at the end of the day, you really need to work with someone who’s going to help examine and process all of the painful shit that has happened to you. You need someone to bear witness to your pain. If you find an energy healer who can do this, fantastic. But, oftentimes, this means going to therapy. And, if you’ve experienced trauma, this often involves doing some intensive trauma work (i.e., going back to revisit and heal what happened to you). If there was another way, I’d tell you about it. Trust me. I’ve tried everything. And, not only do I have access to all of the cutting-edge treatments and tools, I am adept at administering many of them. But, I couldn’t do it myself. I tried for decades to no avail. I finally had to hire a trauma therapist to help me, to bear witness to what I’d experienced. And, thank god I did, because that’s when the real healing began.
The Problems with Spiritual Bypassing, Toxic Positivity and Ableism
I’m not the only one who’s tried to take the personal-growth shortcut. There is actually a term for this; it’s called spiritual bypassing. Spiritual bypassing describes an attempt raise our individual consciousness level without doing the painful heavy lifting to directly address our wounds. So, rather than going to therapy to process our trauma wounds, we begin a rigorous meditation practice, we throw ourselves into a religious practice, we hire a business coach to help with motivation or we try to DIY it with podcasts and self-help books. We may experience some success with these methods, but it’s often unsustainable. Toxic positivity is a very similar concept; it involves ignoring or dismissing negative emotions by jumping right over them and into a positive reframe (e.g., “But look at everything you have to be grateful for!”). The heart of toxic positivity is often in the right place, wanting to bring cheer and make some proverbial lemonade out of lemons, but doesn’t consider the reality of the experience, which is its fatal flaw. Ableism is yet another concept in this family, describing a type of discrimination that favors non-disabled individuals. Ableism is ingrained in our cultural and personal narratives and extends beyond physical disability to include cognitive and mental health disorders. It includes narratives such as, “Just get over it and move on” and “Pull yourself up by your bootstraps” (Wikipedia-Ableism).
Spiritual bypassing, toxic positivity and ableism all bypass the reality of what someone experienced or is currently experiencing, completely missing the opportunity for true empathy; that is, missing the experience of meeting another in the space they are currently occupying. This can leave the other person feeling something therapists like to call, invalidated. The other person feels unseen and unheard, which can lead them to feel even more alone and disconnected than they did before someone attempted to “help” them. And, we don’t just do this to others, we do this to ourselves, completely missing the opportunity to fully be with ourselves in our pain. At the roots of spiritual bypassing, toxic positivity and ableism are often a discomfort with negative emotions and disabilities, an unwillingness to experience them, and/or a fear of contagion, which explain why these experiences are skipped right over and supplanted with more positive emotions or experiences.
Not only do these tactics result in invalidation, they don’t work, at least not sustainably. It’s very difficult to hold a high energy vibration when the pain from our woundings is emitting noise at the lower energy vibrations. We may be able to hold a higher vibration temporarily but it’s unstable and ungrounded, like trying to balance on a tightrope; the slightest breeze can send us careening back down to the lower energy vibrations. In order for a higher energy vibration to stick, it needs to be grounded, it needs to become rooted in us, like our woundings once were. And in order for it to be grounded, we need to heal the wounds that contribute to an unstable foundation.
Spiritual bypassing, toxic positivity and ableism also prevent true healing. In order for true healing to occur, we need to accept our past and present realities, as unpleasant as they may be, and allow ourselves to exist in them for as long as is necessary for change and healing to transpire, for as long as it takes to create a stable foundation. We need to bear witness to our own suffering.
These concepts violate what many of us would assume from a logical perspective; that is, that optimism should be a completely positive influence. As we’ve discussed, however, we can see that optimism can actually be quite harmful when it ignores reality. Concepts such as the Stockdale Paradox and radical acceptance further highlight the potentially damaging role of unbridled optimism; they also underscore the importance of accepting reality, painful as it might be, for both survival purposes and emotional healing.
The Problems with Unbridled Optimism and the Stockdale Paradox Solution
On September 9, 1965, Admiral James Stockdale was shot down over North Vietnam. He was subsequently captured and spent the next 7 ½ years in a Vietnamese prison camp, where he was repeatedly tortured and locked in solitary confinement. He was finally released on February 12, 1973 and went on to receive the Congressional Medal of Honor for his distinguished service and acts of valor (Wikipedia-Stockdale). Experiences such as his, tragic as they may be, provide us with a unique opportunity to understand and harness the power of human resiliency. It is a power of the mind, not of the physical body. In Jim Collins’ (2001) book, Good to Great, Admiral Stockdale related his experiences, observations and mindset during his imprisonment. His mindset utilized what’s called a dialectic. It was a mindset that allowed two seemingly disparate truths to coexist: He never lost hope that he would one day be released and this imprisonment would be the defining moment of his life; and at the same time, he fully accepted and faced the painful reality he was forced to live in. In theory, it sounds simple enough, in practice, it’s nearly impossible to master, a life’s work. This is because as humans, we struggle with ambiguity, we need certainty, for things to be black-and-white, and we especially struggle with feeling two contradictory emotions at once, like optimism and despair. So, when it comes to applying the Stockdale Paradox, most of us vacillate from one pole to the next: from optimism to despair and back again. We have difficulty holding the optimism and despair at the same time. But, Stockdale figured out how to master it, which means that it is not impossible; rather, it means that he has an invaluable lesson to teach us, if we are willing to learn. And, according to the Law of Diffusion of Innovations and Morphic Resonance, as more of us apply and master Stockdale’s paradoxical mindset, the easier it will become for the rest of the population to apply and master.
Stockdale’s observations of the attitudes of his fellow prisoners are also crucial to our discussion. When asked who didn’t make it out of the camp, he succinctly related how toxic positivity played a major role in casualty rates: “Oh, that’s easy, the optimists” (Collins, 2001, p. 85). He went on to explain that these were the individuals who would pin all of their hopes on getting out by Thanksgiving, then Christmas, then Easter, and when they weren’t released as expected on these arbitrarily determined release dates, they’d be crushed, over and over again. These individuals didn’t allow themselves to accept the reality they were currently residing in, they dissociated themselves from it, as a way to cope, by focusing only on their point of escape from the pain. They kept searching for the golden ticket, that one thing that was going to change everything, that was going to save them from their horrific reality. All of their energy went to this, went to living for the golden ticket moment they’d be released. They didn’t focus enough of their energy on how to manage day-to-day survival in a horrible situation, how to live in the present moment. They didn’t ask themselves, “What is this trying to teach me? What can I gain from this experience? What is my purpose here?” These are questions which can turn a hopeless experience into one of empowerment. The optimists just focused on desperately trying to escape their reality. And, when their optimism failed them, repeatedly, they gave up. Rather than focusing his energy in one place, Stockdale divided his energy between optimism and coping with his painful reality, seeing adversity as a test, teacher and vehicle of empowerment; this is likely why he survived. Of the optimists, and his contrasting mindset, he said,
“…they died of a broken heart. This is a very important lesson. You must never confuse faith that you will prevail in the end—which you can never afford to lose—with the discipline to confront the most brutal facts of your current reality, whatever they might be” (Collins, 2001, p. 85).
Stockdale’s wisdom is especial timely during our current state of world affairs. The optimistic mindset that failed his fellow POWs can be seen in the collective’s behavioral response to and attitude towards the COVID-19 pandemic: Eradicate the virus and return to normal life as quickly as possible. We aren’t truly living in the reality of what we are facing. We are simply living for the moment the virus will be eradicated and we can return to life “as normal.” As soon as infection rates begin to decline, we think we’re home free, that we’ve been handed the golden ticket. We remove our masks, stop social distancing and lift restrictions. What the continued infection rates, new coronavirus variants and reinfection rates are showing us is that our current approach is ineffectual and harmful from a survival perspective, especially when we consider the Stockdale Paradox. We will fare much better as individuals and as a culture if we simply accept the fact that the coronavirus isn’t going anywhere anytime soon, realize that we need to adjust our behaviors (and expectations) accordingly, and at the same time, hold hope for a better future, whatever that might look like (Groysberg & Abrahams, 2020). If we don’t, we will have more than a pandemic to deal with, we will have a mental health epidemic on our hands. Unfortunately, we are already experiencing the beginnings of one. Experts in Italy and France are reporting that rates of depression and anxiety have doubled since the pandemic began, and in the United States, the surgeon general has expressed concerns over the adverse effects of the pandemic on mental health (Cohen, 2021).
The Problems with Unbridled Optimism and the Radical Acceptance Solution
Marsha Linehan, the creator of Dialectal Behavior Therapy (DBT), describes a mindset similar to Stockdale’s, required for healing trauma and other emotional wounds. This mindset also underscores the problems with toxic positivity, spiritual bypassing and our response to the pandemic. She called this mindset, radical acceptance. It is exactly what it sounds like, a radical acceptance of our current and past realities, just as they are, like them or not, not as we wish them to be. And, like Stockdale, she elucidates the importance of striving for a better future alongside this acceptance, rather than falling into complete denial, despair and inaction.
“Radical acceptance doesn’t mean you don’t try to change things ... You can’t change anything if you don’t accept it, because if you don’t accept it, you’ll try to change something else that you think is reality” (Linehan, 2017).
The “something else that you think is reality” she’s referring to is the same type of reality the optimistic POWs and COVID-19 optimists were/are seeking, an anything but here, reality. When terrible things happen, we often engage in a sophisticated form of the denial defense, an if only mindset. We don’t necessarily deny that the event happened, we just try to re-write our lives with a better ending (or better current reality), “If only I wasn’t abused, then my life would be better in x, y, z ways,” “If only this virus were eradicated, then…,” and we proceed to live in some variation of this hypothetical reality. Interestingly, this mindset only considers an idealistic future; it fails to acknowledge the possibility that our lives could have actually turned out much worse. Many science fiction writers have depicted these dismal alternate realities in books and movies: Someone goes back in time to change one element of history, and upon their return to the present, they arrive to find a dystopian reality or a world in which they were never born. These stories portray literal changes to historical events, but they also serve as a metaphor to illustrate how we all engage in this revisionist history mindset in our everyday lives but fail to consider dystopian alternatives. The problem with this mindset, is that rather than utilizing our energy to process and heal the pain from the painful event, this mindset directs us to spend our energy trapped in a victim role, wishing the event had never happened, being angry that the event happened, blaming the perpetrator or event (or ourselves) for ruining our lives and in so doing, effectively missing the opportunity to take ownership of our lives moving forward. The event that happened continues to drain our power and controls our lives. This unhelpful mindset is exactly what Linehan is describing in her quote above.
When we don’t face and process the reality of what has happened or is happening to us; that is, when we deny it, we are implicitly sending ourselves the message that we can’t handle it: It’s too shameful; it’s too terrifying; it’s too ugly; it’s too much to bear. Our denial defense is completely disempowering, much like the original wounding experience itself. With our denial, we perpetuate the disempowerment of the wounding experience, perpetuate the narrative that we can’t handle it, and we let the experience continue to have power over us. And, as discussed above, we end up living in an alternate reality of sorts where the experience didn’t really take place. Ultimately, from this place, we can do little to affect positive change in our lives moving forward. Pretending the terrible event didn’t happen or isn’t currently happening can be a useful defense against a short-term stressor and can sometimes be useful for those in positions of complete powerlessness (e.g., children living in abusive homes, people living in institutional settings), but is not a useful long-term strategy (e.g., as a response to a pandemic, as the continued response of an adult who survived childhood trauma) because it requires denying, dissociating, metaphorically cutting off a part of ourselves to maintain the charade. It requires living in a false, alternate reality; and as Stockdale points out, doing so can lower our chances of survival.
Another drawback of utilizing the if only mindset variant of the denial defense is that we end up wishing our lives away. We spend so much of our energy focusing on the time when things will be better, or the version of reality in which this bad thing never happened, that we miss our present reality. Yes, we may have been dealt a shitty hand, and facing the truth of what happened in the past or is happening in the present is painful, uncomfortable and not preferable. But, we just get this one life. Painful or not. There are many people who don’t get to keep on living, whose lives are cut short. We have to make a choice about whether we want to check out mentally (i.e., dissociate) before our time is actually up, effectively leaving us to lead a half-life, or if we want to be fully present in the life we have been given, living it to the fullest. For better or worse. When there’s a lot of pain, this is a tough call. But, when many of us make the choice to check out mentally, we do so unconsciously, and in so doing, we lose our free will, we lose the opportunity to consciously choose whether we truly want to check out or not. The problem with dissociating to escape pain is that we don’t just escape the pain, other negative emotions and negative experiences, we escape all of the positive emotions and experiences too, like love, joy, excitement and miracles. That’s the tradeoff. It is possible to have a miraculous, joy-filled life following painful, traumatic events, but we have to decide to be present and fully accept the pain first. It’s a real mother fucker of a process, but it is worth it.
The mindset required for this process is a dialectical one. This involves both accepting the painful truth of the event, which includes the feelings that come with it (e.g., anger, blame, shame, guilt, grief, pride, fear), while at the same time holding hope for a brighter future and taking steps to change, heal and move toward that brighter future. This future is not a future in which the event never happened, this is a future in which this event no longer has power over us, a future in which we may even find some meaningful lessons in this event, as impossible and perverse as that may seem. When we practice radical acceptance of our painful realities and take practical steps toward change (e.g., ask for help, learn to set boundaries, take better care of ourselves, work on changing our unhealthy behaviors), not only do we see direct change resulting from these steps, we often see change that is indirect, mysterious. In some cases, this change could even be called miraculous. This is change that results from us finding a way to tap into source consciousness, the place from which miracles truly can arise. If we go back to Hawkins’ (2002) conceptualization of consciousness, this possibility makes sense. When we move into acceptance, we raise our energy vibration well above the tipping point of courage (200); we raise it to 350, and with that, we develop a heightened ability to tap into source consciousness, where miracles occur. When we stay in our if only mindset, we are operating from one of the ego’s defense mechanisms (i.e., denial), driven by emotions below the level of courage, which makes it very difficult to access source consciousness and the miracles that arise from it.
The example of miraculous change I’m going to share requires me to be really vulnerable with you. Vulnerability feels dangerous because sometimes people use our vulnerabilities against us, as weapons to harm us. I’m going to trust that you won’t do that to me and trust that even if you do, I’ll be able to handle it. Here goes. Clinical psychology Ph.D. programs are incredibly competitive and difficult to get into, more difficult to get into than medical school (8% vs 45% acceptance rate, respectively; Association of American Medical Colleges, 2008; Norcross & Kuhle, 2011). Many people do not get in on their first try. I am one of those people. I still carry some shame around this because part of me fears this means that I’m not good enough, smart enough, or competent enough to be in this field. Will people respect what I have to say? Will clients trust me to help them? This is classic imposter syndrome. The first time I applied and was rejected, I was devasted. The second time I applied and was rejected, I was beyond devasted. I went to a very dark place. Some loved ones tried to pull me out using toxic positivity, “Don’t worry, something better will come along.” This made me feel worse, as toxic positivity usually does, because they completely missed the gravity and pain of my experience. Some even told me to just give up and try something easier, “Why don’t you just get a Ph.D. in counseling psychology?” This also made me feel worse, like they didn’t think I was good enough either, but it also made me even more determined to prove them wrong.
I allowed myself to fully accept the painful reality of the situation I was in, that I had been rejected yet again, that the odds were against me, and that it would be another year before I could reapply and even then, there was no guarantee I’d get in (radical acceptance). This was incredibly painful because it required me to confront the demons (i.e., traumas) that had erroneously taught me that I was worthless and stupid. Luckily, through the yells of these self-deprecating voices, I heard a different truth. That truth said that I had what it took, that I was good enough. And there was also something in me that wanted this degree so badly that I refused to give up (holding hope for a better future).
This truth was a truth I could feel deep within the fabric of my being, in my bones. It was a resonant feeling, a feeling that made me feel hopeful, nauseated and tearful, whereas the negative “truth,” that I wasn’t good enough and should just give up, produced a dissonant feeling; it made me feel incredibly angry, like I wanted to punch someone in the face. Now that I know more about how my intuition/soul/source consciousness speaks to me, I know that this was my soul saying “yes” to a Ph.D. in clinical psychology and “no” to giving up and settling for something else. I call the resonant “yes” feeling my puke cry, and I get it whenever I know something is true for me. And, whenever I feel like punching someone in the face, I know I’ve gotten a “no,” that I’m hearing an untruth or have experienced a violation (e.g., of my autonomy, of my boundaries, of my values). The voice of truth varies for different people, but here are some common examples in case you are curious about what this might look like for you. Your truth might come in the form of a resonant feeling or it might “ring true” for you; you might feel goosebumps, a chill/cool sensation, a hot flash, a flash/jolt of energy, a feeling of joy/excitement, a funny feeling in your stomach, nausea, tears; your ears might ring; you might laugh when you hear a piece of wisdom or a message; you might hear a small, quiet voice; or you might hear a message in an accent or different language (Ogren, 2019). The voice of untruth or a violation (of autonomy, boundaries, values, etc.) often show up as anger, a violent urge, a gut-punch feeling, or a “fuck no” attitude. Start paying attention to these feelings and experiences when they show up; collect some data about what’s going on at that time, about what you ultimately chose to do, and about how things turned out afterwards. With some practice, you’ll begin to fine tune your intuitive antenna.
When I realized which truth I should listen to, I got to work. I figured out what I needed to do to strengthen my Ph.D. application, and took aligned action: I applied for competitive research jobs and began aggressively studying to re-take the GRE (taking practical steps to make a direct change from the place of radical acceptance). After a few weeks had passed, I got a call from a friend about an opening for a research position in Philadelphia, with one of the most famous psychiatrists in the world, Aaron T. Beck, the founder of Cognitive Therapy. Excuse me? What did you say? Aaron Beck? I couldn’t believe the opportunity that had been presented to me. Just a few weeks earlier, I was a Ph.D. program reject, now this? Oh, how the tides had turned. This was a job most psychologists would give their right arm for, the chance to work with one of the most influential people in the field, THE Aaron T. Beck. I knew the odds were against me, but I applied anyway, because at this point, I recognized that events weren’t transpiring on the rational, third dimensional plane any longer. And, by the power of forces I don’t fully understand and against all odds, I got the job, and began packing up my small town, Midwestern life to move to the big city. I couldn’t believe it, and frankly, I still have a hard time comprehending the entire experience. No Ph.D. program wanted me, but Aaron Beck did. Maybe I wasn’t a complete moron after all. In that moment, I knew that I’d just been handed a golden ticket, that not only would I get into graduate school, that I’d have my pick of career options after I graduated. The miracle didn’t stop there. Shortly after I made it out to Philadelphia, I was selected to work directly with Dr. Beck as an editor on his latest book. And after that, he promoted me to a highly coveted position, to the role of his personal assistant. These were experiences I could have never imagined in my wildest dreams, let alone in my time of despair and rejection from graduate school. I have revisited this story many times over the years, especially when I feel like all hope is lost. It reminds me that even in our darkest hour, miracles can happen.
Now, I know I’ve been talking about how finding the golden ticket turned my life around in my darkest hour, but earlier, I said that searching for the golden ticket was what sealed the tragic fate of the optimists in the POW camp. So, are you supposed to search for a golden ticket or not? Okay, the key distinction here is the word, search. The golden ticket can be what saves us, but we can’t go looking for it. We have to radically accept our current reality, take steps to change it and then let go and let the ticket come to us (but without expecting it to come to us). It’s a complete mindfuck, I know, but it is what is required for the golden ticket to actually show up, if it wants to. We need to be in that higher vibrational energy mindset of radical acceptance. Sometimes we get a golden ticket, sometimes we don’t. If we don’t get one, it doesn’t mean the universe hates us, it’s just means we didn’t get a golden ticket this time. We work to radically accept this fact and we move on. But, when we do get this golden ticket, it is clear to us that something very special has happened, that a rupture in the fabric of space-time has occurred and has allowed something otherworldly to come into the conventional world. This story is a great example what Jung and Pauli called synchronicity and provides evidence for the phenomenon of source consciousness, breaking through into the third dimension (Cambray, 2009).
We also need to understand that although the golden ticket may deliver us from our suffering, if we do not learn our lessons and heal our wounds, we will not be able to anchor into the golden ticket experience or the life we want. So, in my example, my golden ticket was exactly what was needed to pull me out of the darkness I was in and it was what I needed to finally get into graduate school. It even made me feel better about myself: smarter, confident, competent, valuable. But it wasn’t enough. I was plagued with feelings of inadequacy for years after that and suffered greatly in my graduate program because every setback and piece of abusive or negative feedback pulled me back into a dark place. I had not fully healed my wounds and developed a confident, stable sense of self, independent from my external environment. When things were going well and I was in healthy environments, around healthy people, I was fine, but when faced with disappointments, toxic environments (e.g., academia, an abusive marriage) and toxic people, I absorbed those experiences, believed the messages, felt responsible and saw all of this as further evidence that I was a piece of shit, destined to be mistreated and tossed about by the whims of fate. It wasn’t until I did some intensive healing work that I was able to extricate myself from these environments and people, and develop a positive sense of self, independent of experiences, feedback, messages and validation from the external environment.
Ableism and Victim-Perpetration
The Stockdale Paradox and Linehan’s radical acceptance outline a helpful mindset and corresponding actions we can utilize when confronting our painful current and past realities, and they offer a solution to spiritual bypassing and toxic positivity. Unfortunately, spiritual bypassing, toxic positivity and ableism are rampant in the self-help and spiritual communities, and even in the field of mental health, with its managed care (insurance)-driven manualized treatments designed to efficiently relieve surface-level symptoms in 12 sessions. Ableism in particular is so ingrained in our cultural and personal narratives that it pervades even the solutions to spiritual bypassing and toxic positivity I’ve discussed above (i.e., the Stockdale Paradox and radical acceptance). Ableism and its “pull yourself up by your bootstraps mentality” are so ingrained in me that they pervade this entire article, despite my awareness of them. I even provided a couple of examples, Stockdale’s survival of a POW camp and my personal example of overcoming graduate school rejection, that highlight this bootstrap mentality. These examples may perpetuate the belief that if you just try hard enough, your life will be better, which may also imply that when things aren’t good, it’s because you didn’t try hard enough (or are otherwise to blame). This mindset also assumes some level of autonomy and capacity for major change. These are not present in every person and in every situation, so it is inappropriate to apply this mindset universally. Some people are constrained by physical, cognitive and mental health limitations as well as situational limitations, so choice and changemaking may be elusive, if not impossible options.
At the same time, many of us give up too quickly, don’t try at all or use victimhood to avoid doing hard and painful things. It’s a delicate dance between completely collapsing into the experience, jumping over the experience and into something positive, and just being there in the experience. I know on my own journey, ableism and its bootstrap mentality got in the way of me asking for help and didn’t allow me to fully feel the weight of the painful things that had happened to me, which impacted my ability to heal. At the same time, many in our culture use victimhood as an excuse, and also as a weapon, as in the case of victim-perpetration. Victim-perpetration is a term used to describe using a wounded or disadvantaged status to manipulate or control other people, to use this power over them, in order to get personal needs met (e.g., guilting someone into helping). And, this is never okay, to abuse our power or victim status, no matter how much we’ve been victimized. There is definitely a time and place for experiencing victimhood on the journey (not victim-perpetration) and also a time and place to stop letting it have power over us. Where this line falls for each person and in each scenario is not for me to decide.
What Happens When We Don’t Evolve Our Consciousness?
Let’s talk about what happens when we don’t reset our thermostats, when we don’t evolve our consciousness, aside from total world destruction. What does this all have to do with YOU? Well, what this has to do with you is that if you don’t do your work to heal your wounds and ultimately raise your energy vibration, the life of your dreams will have a really difficult time making its way to you. And, if it does make its way to you, it will probably spontaneously combust. Bummer, huh? Remember the lottery winners? Yeah. Double bummer. Not only that, as we’ve discussed, when we don’t do our work, we can harm others, are vulnerable to exploitation and drain energy from the collective in the process. Triple bummer.
In The Big Leap, Gay Hendricks (2009) explains our tendency to unconsciously self-sabotage. When we experience too much positive emotion, we hit what he calls the Upper Limit, which is that set point on our respective thermostats. At this Upper Limit, strange things begin to happen: We get sick before the big date, we get in a car accident on the way to a job interview, we “accidentally” get drunk before our final exam, we close a big deal at work and then go home to have a nasty fight with our spouse, we begin to feel joy and then we start telling ourselves how much we suck and how nothing will ever work out. Back down to “reality” we fall, back down to the devil we know. Let me be clear. We don’t usually do these things on purpose and sometimes these experiences appear completely out of our control, but these experiences are too highly correlated with our potential for happiness to be dismissed as mere coincidence. I know you know what I’m talking about. The Law of Attraction also describes this phenomenon, that we attract what we put out into the world, that our dominant energy vibration predicts the type of reality we experience (Hicks & Hicks, 2006). As discussed earlier, this doesn’t mean that we are to blame for every misfortune in our lives. These concepts are meant as general frameworks for understanding human experience; they do not explain everything.
One way we can reset our thermostats is by healing our wounds and overcoming our fears with the help of therapy. In other words, by addressing the roots of our Upper Limit Problem, or complex, as Jung called it (Singer, 1972). Another thing we can do is to practice tolerating positive emotions. Essentially, we need to do exposure therapy for positive events and emotions the same way we would do exposure therapy for feared events and emotions. Crazy, I know, but humans are funny creatures. As you’ll recall from the discussion of our operating system, Fear 1.0, most of our systems are programmed to see good things and feelings as threatening, so we need to reprogram our systems to see them as safe. We also need to work on changing the old beliefs we have about positive emotions and experiences, those beliefs that show up to sabotage us, talking us back down into the dismal old reality of scarcity and victimhood. In so doing, we begin to see positive emotions and experiences as life giving, rather than life threatening. Guess where you can learn how to tolerate positive emotions and change your beliefs about them? That’s right, therapy! You can also try some of the other options I list at the end.
So, why do we want to reset our thermostats, to overcome our Upper Limit Problem? What’s the end game? The end game is our Zone of Genius: the soul-led, life of our dreams. Our Upper Limit Problem is what keeps us from it (Hendricks, 2009). If we apply Hawkins’ (2002) consciousness model to Hendricks’ concepts of the Zone of Genius and the Upper Limit Problem, we see that the Zone of Genius is akin to tapping into source consciousness at level 500, love, and is soul directed. The Upper Limit Problem is akin to the noise emitted by the lower levels of consciousness (below level 200, courage), which obscures the higher levels of consciousness (Zone of Genius), and is ego directed.
And, although Henrick’s book is written from a career perspective, his concepts can apply to any aspect of life. There are four different zones we can operate in at a particular time, in a particular area of our lives. The titles are fairly self-explanatory but I’ll provide some explanation anyway.
Zone of Incompetence
Tasks in this zone are things you suck at. Or, things you really dislike. Hendricks (2009) says that we should never spend our time in these activities. They elicit negative (lower vibration) emotions, drain our energy, and take time away from doing things we enjoy. In other words, they keep us out of our Zone of Genius and lower our consciousness level. Mowing the lawn falls into this category for me. I hate everything about mowing the lawn: handling the gas, smelling the exhaust fumes, having the sun beat down on me, getting sweaty, getting dirty, experiencing physical exertion, listening to the noise. Hate it. Hate it. Hate it. For years I have mowed my own lawn, dreading it so much that I generally go at least a month between mowings, which as you can imagine, makes my lawn mower very angry and makes the task worse. Frustrating the task further, my lawnmower is a 40-year-old model that my dad found at the local dump and fixed up for me, so it is especially temperamental, prone to overheating, flooding and not starting at all.
Why do I continue to mow? Because I was taught that it’s lazy and extravagant to pay someone to do something you can do yourself; it’s a sign of weakness and incompetence. And, my lawnmower? It runs 75% of the time, so it would be “wasteful” to spend money on a new one. Unhelpful beliefs and behavioral patterns such as these are primarily what keep us locked in the Zone of Incompetence. The last time I mowed my lawn it was 90 degrees out, my lawnmower quit several times, the pull cord didn’t want to work, I ran over a yellow jacket nest, and the lawnmower completely quit working when I had only a 10’x15’ section left. So, I had to get out the hedge trimmers and cut the rest of the grass by hand, on my hands and knees. When I was finished, I was pissed off, collapsed onto the ground melodramatically, cried and proceeded to feel cranky for the rest of the day. Luckily for me, I was reading Hendricks’ (2009) book at the time and saw clearly what had just transpired. I vowed to never mow my lawn again. I would hire someone to do it for me. Mowing the lawn is the worst waste of my time and emotional energy, and it is completely worth it for me to pay someone to do it for me.
Let me take a moment to provide a caveat: Hendricks (2009) says that if a task isn’t in our Zone of Genius, but we really love it, it’s still okay to do it. So, if we love to sing but have a dreadful voice, we should sing anyway, because it’s not draining our energy or eliciting negative emotions (in us anyway). In fact, I’d even go so far as to argue that if we really love something, even if we aren’t great at it (or aren’t great at it yet), it actually has the potential to put us in our Zone of Genius. Using the singing example, I’m sure all of us can think of some examples of terrible singers throughout history who have managed to become famous, who have managed to reach their Zone of Genius, simply because they loved what they were doing so much (e.g., William Hung).
Zone of Competence
Our Zone of Competence includes tasks we perform at a level of mediocrity or tasks from which we derive a moderate amount of enjoyment. Other people can do these tasks much better than we can and these tasks don’t light us up inside. Marketing is one such task for me. For years I’d neglected it, then tried to do it on my own, but just muddled through, never making much progress, with my business suffering in the process. Turns out, marketing is kind of a big deal when you run a business. But, some of the same unhelpful beliefs that kept me mowing my lawn in my Zone of Incompetence also kept me from asking for help with my marketing. I was also taught throughout college and graduate school that marketing is the evil, illegitimate progeny of psychology, who uses the gifts psychology has bestowed upon them to manipulate and control people. So, people in the field of psychology hate marketing. This is fine if you live in academia, but if you live in the business world, this belief is a huge block to success. So, I had some major internal work to do before I could move out of my Zone of Competence with marketing. But, move I did. I went to therapy and took classes to change my unhelpful beliefs, then I hired a marketing person who taught me how to market in ways that were in line with my values (which don’t include manipulating and controlling people). And, you know what? I’ve learned that I actually really love marketing. It’s like cracking a code for me, which puts me into my mad-scientist, Zone of Genius.
But, I spent a lot of time in my Zone of Competence before I got the help I needed to get out. As a result, my business and I paid the price. Indeed, Hendricks (2009) cautions against spending too much time in the Zone of Competence. This is the place where dreams go to die. He observes that people who spend the bulk of their time in the Zone of Competence tend to develop mysterious physical ailments and mental health problems. He suspects that this is because, when operating in the sub-Genius Zones, we are not able to tap into our soul’s energy (i.e., source consciousness), which is what gives us strength and vitality. And, for some reason, these mental health problems and mystery ailments seem especially pronounced in the Zone of Competence. There is a series of science fiction books called The Shadow and Bone Trilogy, which chronicle a group of people with superhuman abilities: the Grisha (Bardugo, 2017). When the Grisha don’t use their powers, they fall ill and begin to languish; when they use their superpowers, they become strong and revitalized. This phenomenon, although science fiction, accurately describes what happens to all of us when we don’t live from our soul’s purpose. This also maps onto what we know about the levels of consciousness. When we operate at the lower levels of consciousness, we feel bad, lacking energy, drive and vitality (we lose our mojo). When we tap into source consciousness, and operate at the higher levels, we feel better, gaining energy, motivation and vitality. And, if we are able to move high enough on the consciousness scale, with a better ability to tap into source consciousness, we develop superhuman abilities, just like the Grisha.
Zone of Excellence
This is where most of us live. Our Zone of Excellence includes tasks at which we excel and may even feel contented performing. We are comfortable here, we’re good at what we do, life is predictable, we are dependable, and others generally want us to stay here because we bring value and stability from this place. However, as much as we may excel, we are not tapping into our soul’s wellspring, into source consciousness. And, ultimately, we will languish in this place of contented excellence. The deterioration will be less pronounced and rapid than the deterioration in the lower two zones, but deteriorate we will. Put plainly, this is the place where dreams go to die, slowly. Because there is such a gradual decline, most of us don’t realize what’s happening until we wake up one day and realize that much of our life has passed us by. This is often when we have the proverbial midlife crisis. We will most definitely get nudges from the universe along the way, urging us to make the leap into our Zone of Genius, but we are usually so comfortable and content in our Zone of Excellence that we rarely listen. Sometimes, when we don’t listen to the nudges, the universe will drop kick us into our Zone of Genius with some really painful life events or mistakes (Hendricks, 2009). If this happens, I strongly urge you to heed the warning. The universe was kind enough to do this for me. I talk more about my personal journey into my Zone of Genius here.
For my neighbor, John, being a medical doctor is in his Zone of Excellence. He likes his work, he’s good at what he does and he brings stability and value to his family from this place. From the outside looking in, you’d assume that he’s functioning in his Zone of Genius; after all, who wouldn’t love to be a medical doctor? He has the career so many of us only dream of. Not only that, he’d have to be really passionate about his job to devote so much time, money and energy to it. But, if you asked John, you’d learn that practicing as a medical doctor is not in his Zone of Genius. He’d tell you that “being a troll" is actually what lights him up inside, is actually the role that puts him in his Zone of Genius. (If you are unfamiliar with the term, troll, it’s what the kids are calling someone who intentionally incites others for their own amusement, using “inflammatory, insincere, digressive, extraneous, or off-topic” messaging; Wikipedia-Internet Troll). He loves to be a disrupter, to say and do things that shock and shake up the status quo. But, being a troll isn’t really “a thing,” well, at least not a thing you can get paid for, so has John quit his day job to skulk about the shadows of the internet? Or, is he slowly fading away, languishing in a hospital job somewhere? No, he’s actually found a way to get paid to be a troll at his hospital day job. Seriously. He’s taken on an HR role at the hospital, where it’s his job to give other medical professionals really blunt and unpleasant feedback. Most people would hate this job. But, he’s completely in his element. And, surprisingly, the medical professionals on the receiving end are actually able to accept and respect the feedback he gives them, which is not a typical response. He’s happy and they’re happy (well, as happy as you can be receiving blunt, negative feedback). It seems almost miraculous, but that’s what the Zone of Genius is all about.
Why do people stay in their Zone of Excellence? For the same reasons we stay in the other zones: our unhelpful beliefs, our egos, a variety of sociocultural factors, and a social psychology phenomenon called, the sunk cost fallacy. The sunk costs fallacy states that when we put a significant amount of time, energy, or money into something, we are more likely to stick with it, even when the costs outweigh the benefits. This is part of the reason why people stay in abusive relationships (part of the reason, there are many complicated reasons). They’ve put so much time and energy into making the relationship work and have endured so much pain and suffering that it’s difficult to walk away. Their brain tells them, “It must really be worth it if you are willing to go through all of this,” and so they stay. Careers in our Zone of Excellence generally involve a high level of temporal, energetic and/or monetary investment: We’ve spent 20 years in the field, perfecting our craft; we’ve put our blood, sweat and tears into our work; we have a mountain of student loan debt. Plus, we feel relatively satisfied here (and, if it ain’t broke, don’t fix it). For these reasons, the sunk cost fallacy says we will have a difficult time leaving our Zone of Excellence. There are, of course, other reasons why we have difficulty making the leap to our Zone of Genius. We will discuss those later.
Zone of Genius
This is your calling. Your soul’s desire. The tasks in this zone energize you and bring you joy. If you are working in your Zone of Genius, it won’t feel like work, it will feel like fun. This is what you would do with your time if your bills were paid in perpetuity and you had no obligations. We’ve already talked about John, and his Zone of Genius position as an HR troll. What’s mine? Being a mad scientist wizard. It’s okay if you don’t think that’s a thing. In fact, that’s kind of the point. The Zone of Genius is all about moving outside of the box prescribed by polite society and into the undefined creative space that makes your soul happy. A few years back, when I was drop kicked into my Zone of Genius, I stopped practicing as a traditional therapist and went rogue, forgoing licensure and pursuing esoteric practices, like dream interpretation and the use of extrasensory perception. I also started to spend a good portion of my time researching, writing and inventing. I’ve never been happier and my clients are seeing better results. Want to know the other wild thing about living on your Zone of Genius? You can actually change how time moves. What? Yeah, it’s called Einstein Time and it basically means that we become masters of the universe (Hendricks, 2009). While on Einstein Time, we begin to experience space-time as it truly is, not fixed and bound by gravity, as it’s typically experienced on Earth. Time begins to expand for us. As cool as this topic is, it is a rabbit hole I’m going to have to save for another time, perhaps another article (or a book?). Stay tuned.
You’ve probably heard of the Great Resignation, which is the term used to describe the phenomenon of increased rates of voluntary resignation despite increased rates of unemployment that began in the spring of 2021. The Great Resignation is a function of people taking stock of their lives, recognizing that the drawbacks and risks of their jobs (e.g., wage stagnation, time commitment, poor and unfair working conditions) outweighed the benefits, realizing that their current jobs weren’t fulfilling them, and that there were other aspects of life that were more important (e.g., health, family, enjoyment; Wikipedia-Great Resignation). The Great Resignation is also a great example of people clearing their paths so they might make their way into their Zone of Genius, whether they are fully conscious of this fact or not. In other words, the Great Resignation has provided a unique opportunity for more people to move into their Zone of Genius, tap into source consciousness, and in so doing, help themselves and humanity in the process.
Are You Living in Your Zone of Genius?
Now for the million-dollar question: Are you living in your Zone of Genius? Here’s the deal. Very, very few people in America are living in their Zone of Genius. It is the antithesis of our cultural narrative. So, even if you think you are, I challenge you to get really honest with yourself. Begin by asking yourself the following questions and pay attention to your immediate answers. By “immediate answers,” I mean the answers that show up within 500 milliseconds. Anything that shows up after that is your conscious, ego mind, trying to rationalize your current life choices in order to keep you playing it safe, small and status quo. Here are the questions:
Are you excited to get out of bed in the morning?
Do you love your life?
Do you look forward to your workday?
If you answered with an enthusiastic, “Yes!” Or said, “Yes, that’s true about 90% of the time.” Then, you are likely already living in your Zone of Genius. If you answered with, “No,” “Meh,” “I don’t know,” “I’m happy enough,” “I’m better off than most people I know,” “I’d be happy if…,” “No, but I just can’t make the change right now,” then you are most definitely not living in your Zone of Genius. And, it’s time for you to decide if you want to continue playing it safe, small and status quo (and slowly fade away), or if you want to make the leap into your Zone of Genius. “Do you want to be delighted with your life or contented with it?” (Kretchmer, 2018). (Or, dreading it? Or, numb?) It’s up to you.
Identifying Your Zone of Genius and Barriers to Its Identification
If you are ready to make the leap, contemplating making the leap or if you are simply curious about what your Zone of Genius might be, you can ask yourself the following questions:
“If you could wave a magic wand and do anything with your life, what would it be?”
“If your bills were paid in perpetuity and you had no obligations, how would you spend your time?”
If you answered, “I’d do nothing,” this is a sign that you are exhausted from living in your current (sub-Genius) zone and from navigating the toxic culture we live in. You need some downtime to rest and restore your energy. You may need to voluntarily take some time off from work and other obligations, or at least scale back your responsibilities before your body gives out by getting sick, before your mind breaks down, or before other mysterious circumstances show up that force you to stop, rest and restore. There may also be some internal work that needs to be done in order to clear away the blocks that are standing in the way of your Zone of Genius. After you’ve taken the time you need, come back to these questions. Who knows, maybe you’ll still get the same answer, “Nothing.” And, if that’s the case, I’m sure you can lead a full, invigorating life of doing absolutely nothing.
I remember a time, a few years back, when I was living in my Zone of Excellence, when my primary goal was to retire in 3-5 years. I couldn’t conceive of another 30 years in the workforce. There was no way I’d make it that long without having a nervous breakdown or dropping dead. And, because I have extraordinary skills of deduction, I was able to devise a plan to make this early retirement goal possible. Seriously. Maybe I’ll write an article on it at some point for those of you who are curious. Anyway. Before I could retire, the universe burnt my Zone of Excellence to the ground and I had no choice but to cut back my hours, do a major overhaul of my mental health and completely change the way I worked. Could I afford to cut back my hours? Umm, not even close. I was destitute and had no safety net. Did I want to do intensive PTSD treatment? Fuck no. It was excruciating, exhausting and expensive. Did I want to change the way I worked? Not a chance. I’d spent almost two decades studying the traditional methodology and career practices of psychotherapy, and I didn’t have the bandwidth to start over and learn something completely new (the sunk cost fallacy). But, I was lucid enough to know that when the universe sends a sign that says, “Wake the fuck up and get your shit together,” I needed to wake the fuck up and get my shit together because the next “sign” was going to be much worse. It’s been four years since then (2018), and although I certainly don’t have it all figured out yet, I’m happier, healthier and freer than I was in my previous life. And, I have absolutely no interest in retiring. I love the work I do and know that the world needs my unique gifts. I wouldn’t feel fulfilled and energized if I quit and sat on a beach for the rest of my life.
If you answered the Zone of Genius questions with, “I don’t want to do anything. I just want someone else to take care of me or rescue me.” We’ve all been here. The idea of someone else taking care of us and our lives sounds pretty nice. But, in actuality, it’s not very satisfying and it can be pretty disempowering, stunting our growth. Sometimes, we really are dependent upon others to take care of us, at least in part: when we are children, when we have certain physical, cognitive or mental health issues, when we don’t have the financial ability to support ourselves, when we are trapped in abusive or oppressive environments, when we are institutionalized, when we are imprisoned or enslaved. These circumstances make it incredibly difficult, if not impossible to act autonomously and make change.
But, in many cases, when we are in a perpetual state of wanting to be rescued or taken care of, what has happened is that we’ve experienced abuse and neglect. We come from a family and/or cultural system that didn’t meet our physical and emotional needs; we didn’t have adequate caretaking when we were helpless and in need of caretaking. As a result, not only did our needs go unmet, we also didn’t learn how to meet our own needs adequately because we didn’t see that behavior role modeled to us. So, as adults, we might not know how to complete basic tasks like cooking and cleaning, we might forget to eat, might have trouble budgeting money, might become disorganized easily, we might become easily overwhelmed and emotionally dysregulated, we might not take care of problems until there’s an emergency, and so on. When we grow up in these environments, as adults, we also have trouble trusting that our needs will be met in the future, even if we have lots of evidence stating that they will. This can lead to feelings of panic and anxiety, especially during periods of uncertainty. So, as adults, when we find ourselves falling into a desire to be taken care of or rescued, what is likely happening is that we’ve fallen into an old programming loop, created in an abusive or neglectful childhood, where we are constantly searching for a caregiver in the outside world to meet our needs but are unable to find one.
The trouble is, when we become adults, no one wants to take care of us anymore. People in our culture assume we should be able to take care of ourselves, even if that’s not the case. We should have a culture that feels compassion for the needs of adults and has adequate social programming in place to help, but we don’t. That’s just the truth of it, unattractive as it may be. So, unfortunately, in our current system, we can have compassion for the helpless place we are in, but we also have to be realistic and radically accept the current state of the culture. We have to understand that no one is coming to rescue us, no one is going to take care of us (at least it’s very unlikely that they will). The best we are going to get is help, but we will need to ask for it and we will need to pay for some of it. We’ll need to heal our wounds, face our fears, change our old belief systems and learn the skills we need to take care of ourselves. Most importantly, we are going to have to make a commitment to not give up on ourselves, to not repeat the abuse and neglect that happened to us as children, when the adults in our lives gave up on us and didn’t take care of us. As we do this, the collective needs to work to develop a sociocultural system that cares about and adequately addresses the needs of both children and adults, who need extra help. It’s the collective’s responsibility to stand up and speak for those who don’t have power and who can’t speak for themselves, including Mother Earth (although I’d argue that she’s actually speaking to us pretty loudly with her fires, plagues and floods; we just aren’t listening).
Further Identifying Your Unique Gifts and Zone of Genius
If you answered the Zone of Genius questions with an action word or job title, even a fictitious one, fantastic. Proceed to the following questions. They will help you further identify your unique gifts and ultimately, will delineate your Zone of Genius. Ask yourself:
“What’s my superpower?”
“What do I excel at?”
If you come up with something general like “problem solving,” dig deeper and ask:
“What is it about me specifically that makes me so good at that?”
“What’s a good example of me using this superpower?”
“How do I uniquely display this skill?”
“If the apocalypse arrived, what would I bring to the table? What skills would help me and others survive?”
When I was first trying to figure this out, the general concepts I came up with were problem solving and reading situations, events and people. After digging deeper, I discovered that what it is about me that makes me so good at reading situations, events and people is this: I just get these knowings about them, certain feelings, thoughts, images or memories pop into my mind, or I have dreams about them that provide me with additional information. When I explored this further, I realized it fell under the category of extrasensory perception, so I included this on my list of superpowers along with MI6-level deductive abilities (the type of problem-solving skills I possess). So, spend a little time figuring out what your unique and specialized skills might be. If you get stuck, you can ask friends, family members or coworkers to help you answer these questions.
What If My Zone of Genius Dreams Are Impossible?
So, what if you said that your soul’s desire is to become an Olympic athlete, but you’re middle aged and you’ve never trained a day in your life? Huh? Good question. All I have to say to you is this, “🎵Some people say they know they can’t believe...Jamaica, we have a bobsled team 🎵” (Worl-A-Girl, 1993). Good luck getting that song out of your head today. In case you missed the point: Where there’s a will, there’s a way. If you really want to become an Olympic athlete, I bet you can find a way to make that or an iteration of that, happen. Yes, I know what I’m saying is ableist but I’m also not sure where the line is between pushing you to remove the stubborn egoic and societal blocks in your way and which blocks may prove impossible to remove. In other words, it’s possible that your dreams are impossible and it’s also possible that they aren’t impossible. You’re welcome for that riddle of a non-answer.
I want to come back to what I said about finding a way to make your dream or an iteration of it come true. This brings up an interesting point about how source consciousness/god/universe answers our prayers and requests. We often get what we ask for but what we get might look a lot different than our human minds were originally able to conceive, so we can miss it. For example, when my niece and I were practicing our manifesting magic last summer, she said that she wanted to manifest a flower garden down by the lake. When she said that, I thought, “This isn’t going to turn out well because I know for damn sure there’s no flower garden down by the lake.” When we walked down to the lake, not surprisingly, there was no flower garden there and my niece was visibly disappointed. Because I was motivated to alleviate her disappointment, I tried looking again, racking my brain for a way to find her a flower garden, and here’s what I saw: A huge patch of waterlilies blooming right near the water’s edge, a floating flower garden. Feeling relieved, I said to my niece, “I know it doesn’t look like what we expected, but there’s actually a flower garden right there. Do you see it?” She thought about it for a second, nodded in recognition and then got really excited that her manifesting magic had worked. I’m sure all of you can think of some examples like this from your own lives. I hope you can keep those in mind when you are practicing this whole spiritual, soul-living, Zone-of-Genius thing. The things we ask for may look different (and even better) than we imagined.
What About People Who Don’t Have the Luxury of Moving Into Their Zone of Genius?
I bet you’re wondering how Hendricks’ (2009) Zone of Genius concept applies to children trapped in abusive homes; people with certain physical, cognitive or mental health issues; individuals living in poverty or without the financial ability to support themselves; people trapped in abusive, oppressive or otherwise toxic environments; individuals who are institutionalized, imprisoned or enslaved; etc. Good question. I can’t speak for Hendricks but it was my impression that the book was written for people who had some level of autonomy and for whom change was a viable option. For the folks mentioned above, these conditions may not be met. This doesn’t mean change is impossible. Sometimes, it is in our darkest hour, when we are at our most helpless, that we are able to reach deep within, connect with our soul’s truth and find the strength we need to keep going or build a new life for ourselves. That said, it is still incredibly unfair and ignorant to say that all people’s problems would be solved by simply making the leap into their Zone of Genius. In many cases, a complete overhaul of our sociopolitical, educational, economic, medical, mental health and cultural systems is necessary for these individuals to live better lives and even if that happens, their lives still may not improve.
I would also argue that it’s incumbent upon those of us who do have some level of autonomy and for whom change is a viable option to do the work necessary to heal our wounds, raise our consciousness level, move into our Zone of Genius, and ultimately make the world a better place for others. If you are reading this, there is a good chance you are one of these people. That is because, to read this, you would need to be safe, healthy and financially secure enough to have the luxury of free time, you would need the resources necessary to obtain internet access, and would need a nervous system that’s not so focused on survival that it can free up energy to consider topics like personal growth. Even if you can't make large changes, there are definitely some small things you can do, which we’ll talk about more when we discuss Jupiter Time, therapy, therapy alternatives and complimentary practices.
How the Societal Organism Keeps Us Trapped in the Lower Zones
The Eagles sang, “We are all just prisoners here of our own device,” but that’s not entirely true (The Eagles, 1977). Certainly, we play a role in our imprisonment, but larger factors are at work here. We are a nation founded on slavery and indentured servitude. Between 50-67% of the people who arrived in Colonial America were indentured servants (PBS) and 24% of the population were enslaved (Bourne, 2008).
These numbers, of course, do not take into account the subjugated position of women in our culture, which is likely because this is not a well-acknowledged fact, even today. So, I’m going to take a moment to acknowledge this. Consider these facts: Women didn’t receive the right to vote until 50 years after male slaves. Women weren’t allowed to manage marital property or obtain a line of credit without their spouse’s consent until 1970—1970!? (Crittenden, 2006). Unmarried women weren’t allowed to legally obtain birth control until 1972 (Eisenstadt v. Baird, 1972). And, until 1988, it was completely legal to deny housing to unmarried women with children; such housing discrimination continues even today, albeit illegally, with women of color being the most significantly impacted (U.S. Department of Housing and Urban Development, 2016). These laws are just the tip of the subjugation iceberg; there are many more laws like these and many more discriminatory and oppressive cultural practices that continue to affect women and especially women of color, at present day. The critical thinking points I want to highlight are these: What do these facts tell us about how women are perceived in this culture? What do they tell us about how women of color are perceived in this culture? And how do they continue to influence the mindset and drive the behaviors of this culture?
These facts are disturbing, the statistics are staggering, and their continued influence on our culture’s mindset and behavior is insidious. Unfortunately, I was unable to find a statistic that reflected the proportion of the population under indenture during the same time frame as the statistic that documented the proportion of population that was enslaved, so I can’t say, “In 1790, 74-91% of the population were either enslaved or under indenture, and of the remaining ‘free’ population, 50% were women, so actually, 87-95.5% of the population were enslaved, under indenture or were the property of a man.” But, what I can say is that in 1790, 24% of the population were enslaved and a very large portion initially entered the workforce as indentured servants (Bourne, 2008; PBS). And, the entire female population, roughly 50% of the total population, were either enslaved by plantation owners or were enslaved by a sociopolitical system that considered them to be the property of their husbands or fathers. This means that an astronomical proportion of the population were enslaved, under indenture, were the property of a man, or were descendent from ancestors who were not free.
Today, although most of us have been released from those legal bonds, I would argue that the master-slave and master-servant narrative still pervades our culture, sociopolitical structure, economic system, educational system, medical system and our workplaces. It’s a narrative that says, “Your employer (or husband or father) owns you; your value comes only from the work you do,” “work requires sacrifice,” and, "women's work has no financial value." It’s a narrative that produces terms such as “mandatory” in reference to employment tasks, one that effectively utilizes force and fear to manipulate employee behavior with the implicit message, “If you don’t do exactly what we want, when we want it, there will be some very unpleasant consequences.” This may seem like the definition of a “job” to many of us, but it’s a pretty fucked up definition, if you really consider it. It completely eliminates autonomy. It discourages pleasure and encourages hard work and sacrifice, and it’s used as a method of control, draining the energy of workers and fueling the larger societal organism, especially benefiting those in positions of power (Hawkins, 2002). In addition to these cultural narratives, if we consider the research suggesting that trauma in one generation can change the DNA structure of those in future generations (Hollis, 2013; Selimbasic et al., 2012; Snyder et al., 2016; Youssef et al., 2018), we could even argue that we still carry the enslavement and servitude trauma of our ancestors in our DNA, in every cell of our body, further compounding the impact of this cultural narrative.
Take a moment to consider how free many of us really are. How free do any of us feel to pursue work or activities we truly enjoy? How many of us feel free to take time off, even just a few hours for a doctor’s appointment? How many hours a week do we work, compared to other developed countries? How much vacation time do we get (or take) each year, compared to other countries? How many times have we gone into work when we are sick (pre-COVID), because we didn’t want to appear uncommitted or let work pile up on our desks? How often is the word mandatory used by our employers? If you lost your job or wanted to quit today, how long would you be able to pay your bills?
Europeans work 19% fewer hours than Americans (Bick, Brüggemann, & Fuchs-Schündeln, 2016). The United States is one of the only countries in the world that doesn’t guarantee paid vacation time, and has no yearly vacation requirement (even China requires workers to take 1-5 days of vacation each year; Wikipedia-List of Minimum Annual Leave…). Americans are also one of the least likely groups to use their vacation days, completely forfeiting 768 million vacation days in 2018, for a loss of 65.5 billion dollars in benefits, and taking fewer overall vacation days than pretty much any other country in the world: 10 days versus 25 in the UK, by comparison (Baran, 2018; Kim, 2019). Further, 45% percent of Americans have absolutely no savings, and 69% have less than $1000 in savings (Huddleston, 2019). It’s no wonder we spend the majority of our waking life at work. We can’t afford not to. We are afraid not to, because if we lost our jobs tomorrow, we understand that many of us are just a month or two away from foreclosure, bankruptcy and even homelessness. We feel trapped and many of our employers know this. We may not be under the same type of indenture or enslavement as early colonists, but we are under indenture to the banks, credit card companies, student loan lenders, utilities companies, our landlords and automobile lenders. Even if we are among the lucky few who do have the luxury of financial stability, our cultural narratives discourage us from living a life of joy and pleasure, and instead, encourage a Puritanical work ethic, with its resultant life of duty and obligation (hence why we forfeit vacation time rather than use it). Indeed, even the employers, who are in positions of power, report that they don’t feel they can leave their work behind to take a vacation, take a few hours off on a Friday, take sick leave or early retirement. These narratives have transcended the original players in the game (i.e., master-slave/servant, employer-employee) and now pervade the entire, autonomous sociocultural organism.
So…if you wanted to quit your job tomorrow and live the life of your dreams, as discovered by your answers to the Zone of Genius questions above, could you? If you wanted to give up your responsibilities, your obligations, so that you could start living from a place that made you happy, could you do it? Would you do it? Why or why not? Take some time to answer these questions.
I’m guessing that some of you are having trouble believing that a life lived in your Zone of Genius is possible. Understandably so. Even though slavery, indentured servitude and female subjugation are no longer legal, there are still a plethora of sociocultural, political, economic, educational, medical and psychological factors that continue to restrict our freedoms and lead to the complete loss of freedom for some (e.g., incarceration): a toxic sociopolitical structure, unstable and unsafe housing, major barriers to employment, illiteracy and lack of education, wealth inequality, institutional racism, internalized misogyny, financial slavery, lack of access to adequate medical care, a mental health crisis, lack of effective social welfare programs, cultural narratives that promote scarcity, cultural narratives that discourage rehabilitation, a “justice system” that’s punitive rather than redemptive, ineffectual rehabilitation programs, and lack of adequate funding for social welfare, mental health and rehabilitation (Benecchi, 2021; English, 2020; Smith, 2017). Although most of us are never actually incarcerated, we can still feel the force of these imprisoning sociocultural factors and still they drive many of our behaviors, usually without our conscious awareness. This culture we live in has contributed to our woundings, our fears, our beliefs about self, others and the world, and ultimately, has shaped how we show up in the world. It’s no wonder few of us ever feel free enough to pursue the life of our dreams, why we never feel free to enter our Zone of Genius.
The Hamster Wheel: How Our Fear of Freedom and Our Exhaustion Keep Us Trapped
The fact is, many of us are living in a prison without ever seeing prison walls. When it comes to complete sovereignty and living the soul-led, life our dreams, the societal odds and cultural narratives are against us. Not only that, we are terrified. When we see that glimmer of freedom, we also see its shadow, the devil we don’t know, and many of us don’t want to dance with that devil, the devil of uncertainty. Remember our operating system and its micromanaging supervisor, our ego? Uncertainty is a huge survival risk, there are too many unknown pitfalls and unpredictable pathways for the ego to compute, so it just goes into lockdown mode, ensuring that nothing other than status quo programming can run. A prison might be a prison but it’s also a container, a locked secure place, with structure and predictability. We might not be able get out but nothing unexpected can get in to harm us either (at least that’s what we tell ourselves). So, we stay there, in the life we know, seemingly safe and secure, in our comfortable, structured place of certainty.
Many of us also understand that freedom requires a great deal of work and even if we do want it, most of us simply don’t have the energy. Our culture’s impossible-to-meet financial, societal and familial obligations have drained us. All we can do is keep repeating our well-established routines, punching the clock and living for the weekend. Our lack of energy is compounded by the sunk cost fallacy, discussed earlier. We’ve already put so much time, effort and money into living in our sub-Genius Zones that we can’t justify the cost of abandoning them, only to incur additional costs—time, effort and money—to try something new, even if it holds the promise of a utopian future. As Sheldon Kopp put it, “Everything good is costly, and the development of the personality is one of the most costly of all things. It will cost you your innocence, your illusions, your certainty” (Kopp, 1972, p. 10).
So, when it comes to overcoming our Upper Limit Problem and making the leap of faith into our Zone of Genius, that promise of freedom isn’t enough to wake most of us up and affect major change. In fact, as we’ve discussed, that taste of freedom can actually be so terrifying that it sends us racing back to the relative comfort of prison walls. Further, even if we desperately desire freedom and gather the requisite courage, the sociocultural, political, economic, educational, and psychological factors and societal narratives we have discussed fight us every step of the way.
The Force That Will Set Us Free
So, what’s it going to take? What is powerful enough to catalyze extraordinary change and fight the forces attempting to sabotage it? What could give us the energy and the ingenuity we need to make these changes? What could give us the courage we need to heal our wounds, make major changes and venture into the terrifying land of uncertainty?
By far, the most powerful force I’ve ever seen is, LOVE. This is where the magic happens, and Hawkins’ (2002)consciousness scale would agree. Love has the power to give us energy, joy, courage, compassion; provide us with ingenious solutions; and even give us superhuman powers. And, If I’m being completely honest, the primary reason I got my shit together, dealt with my trauma, changed my life and moved into my Zone of Genius wasn’t because I was afraid of the universe burning my life down again or because I wanted freedom (although these were pretty powerful motivators), it was for the chance at love. When my prison walls came crashing down, I saw the glimmer of something I’d given up on many times in the 20 years prior: true love. I’d had so many disappointments that I just didn’t think it was possible for me, so I’d settled into the Zones of Incompetence and Competence in that area of my life. But, when I saw that glimmer again, it gave me hope. And, I knew I needed to make some major changes or it would evade me yet again. Like the lottery winner example, I knew I needed to grow into a new story with love, which involved doing some deep healing work, if I wanted to hang onto it and stop attracting abusive partners.
I’ve seen a similar phenomenon with clients. They’ve been trapped and in pain pretty much their entire lives but they don’t call me until they see that their pain is harming those (or what) they love most: their kids, grandkids, partners, friends, siblings, parents, themselves, their life’s work or their cause. They use the power of love to amass the courage they need to face their fears, heal their wounds, make major changes and venture into uncertainty.
I think it’s clear to all of us that we have a massive problem on our hands and if we don’t address it promptly and aggressively, the inconveniences we’ve experienced as a result of the COVID-19 pandemic will seem like a beach vacation compared to what will come next. Typically, this is the point at which most folks get overwhelmed, say, “We’re fucked,” and proceed to do nothing. I am encouraging you to do better than that. We need to do better than that.
“We have an opportunity for greatness which has never been offered to any civilization, any generation in human history, to act as a generation to do the right thing. If we fail to act on it, we will become the most vilified generation in human history.” (Payne, 2006)
So, What Can We Do to Affect Change in Ourselves and Ultimately, the World?
Start Living on Jupiter Time.
I know it’s a huge cliché, but start small, start by making a commitment to make a small change each day, to move toward your Zone of Genius, to heal yourself and help the collective (including the planet). If you make small, manageable goals, you are much more likely to actually reach them. And, if you want to do it one better, you can write your goals down. Research shows that people who wrote down their goals were more like to achieve them than those who didn’t (Matthews, 2007).
There’s a concept my mentor, Dr. Marilyn Steele, taught me about called, Jupiter Time. Jupiter is the planet of expansion and miracles, so when you enlist Jupiter’s help, he helps to expand the energy and resources you’ve already contributed to your goal (and then he adds a little magic). To live on Jupiter time, you start with a small goal, something seemingly infinitesimal, then you let Jupiter work his magic. For example, you could set a goal to meditate for 5 minutes a day, to devote 10 minutes each day to study your passion of astrology, to spend 5 minutes each day signing petitions and sending letters to Congress advocating for social justice, to spend 10 minutes each day being a fully present parent. It may not seem like much initially, but 10 minutes each day adds up to 61 hours each year! You can accomplish a lot in 61 hours. And, that’s before Jupiter has worked his magic. With Jupiter’s help, you’ll find that the 10 minutes each day grows into 30 minutes, into an hour, into eight hours, and before you know it, you are living out your biggest goals and desires on Jupiter Time; you have officially made the leap into your Zone of Genius.
How does Jupiter Time work? I have a few hypotheses. One is that making small commitments to change allows us to circumvent our ego. If you recall, the ego is the micromanaging supervisor of our operating system, Fear 1.0. Whenever change is detected, it is ego’s job to step in to ensure that change doesn’t happen, because big changes are seen as big threats. Ego wants us to keep playing it safe, small and status quo. Small changes are dismissed by the ego as trivial (and your ego may say as much when you try to live on Jupiter Time), and therefore, you should be able to implement these small changes without too much ego resistance. Another hypothesis is that this exercise works as an exposure therapy of sorts. The reasons you aren’t currently making changes likely has to do with old stories, fears, beliefs and wounds that are standing in the way of making the changes. This exercise requires you to engage with these old stories, fears, beliefs and wounds, in small doses, each day, until they start to disintegrate. As you are exposed to them, your body and mind learn that the old stories, fears, beliefs and wounds aren’t as threatening as your ego made them seem, and soon you begin to feel safe making the changes. My final hypothesis is that magic, like actual magic, is responsible for making “Jupiter Time” work. In actuality, it’s likely a combination of all three factors that contributes to the success of Jupiter Time.
Go to Therapy
Go to therapy: Heal your wounds, fears and rewrite those old stories and beliefs. Hopefully, at this point, I’ve sufficiently underscored the importance of addressing your pain with therapy and other types of deep healing work. So, what are you waiting for? Get online, and start researching therapists! Psychology Today is a good place to start, Therapy Den also has a good directory. I could write an entire article on what to look for in a therapist and maybe I will. For now, I’d recommend finding someone whose words resonate with you, trust your gut and if you don’t connect with the person you find initially, keep looking. Don’t get too hung up on their training (e.g., EMDR, CBT, ACT). Ultimately, you want a therapist who has a high energy vibration, who has done their own therapeutic healing work; this will help ensure that they won’t project their unresolved issues onto you (called “countertransference”) and that they have the capacity to help you raise your own energy vibration. If they’re really evolved, they may even have spontaneous healing abilities. Research has shown that type of therapy (e.g., EMDR, CBT, ACT) doesn’t matter as much as what are called nonspecific factors, which are factors that are not specific to a certain type of therapy (e.g., cognitive restructuring is a factor specific to a type of therapy, CBT; empathy is a factor that’s not specific to a particular type of therapy). Instead, these nonspecific factors are dependent upon the individual therapist and include warmth, respect, unconditional positive regard, a good therapeutic relationship and a belief in client success (Luborsky et al., 2002; Wampold, Minami, Baskin, & Tierney, 2002; Wikipedia-Dodo Bird Verdict).
So, again, pay attention to your intuitive gut when reading therapist bios and when meeting with the therapist you choose: How do they make you feel? What do you notice showing up in you when you are interacting with them? What do you think this is about? You can also use the truth/intuition testing information I gave you above to determine if this person is a “yes” or a “no” for you. Best of luck!
If I’ve been speaking your language and you’d like to learn more about working with me, you can visit my website or schedule an appointment here. My healing practice is dedicated to finding and freeing executives and intuitives who feel lost and trapped in their normal lives, so they can reconnect with their true north, feel joy and experience magic in their lives. I am located in Minnesota and offer online appointments to clients nationwide.
I’m also going to include a list of therapists/mentors I’d recommend, people who have done their internal healing work and who have higher energy vibrations. Many of them offer online services, but state licensing regulations require clients to be located in the therapist’s state of licensure. I’ll include each therapist’s geographic availability.
Dr. Marilyn Steele: located in California, can see clients located nationwide.
Dr. Nika George: located in Nebraska, can see clients located in Nebraska.
Dr. Jason Drwal: located in Iowa, can see clients located in Iowa.
Donna Corbett: located in New York, can see clients located in New York and New Jersey.
Dr. Emily Strang: located in North Carolina, can see clients located in North Carolina: dr.emilystrang@outlook.com
Try Some Therapy Alternatives and Complimentary practices
I know that I keep joking-not-joking that therapists are going to help heal the world, but it’s not just therapists who are going to help. There are a lot of people in other professions working to heal the world and they deserve to be mentioned: energy healers, shamans, psychics, mediums, social workers, yogis, physical therapists, massage therapists, Reiki practitioners, acupuncturists, teachers, chiropractors, pharmacists, medical doctors, nurses, midwives, mothers, fathers, artists, lawyers and environmental advocates. I know I’m forgetting some, so please let me know if I should add your profession to the list.
If you aren’t willing, able or ready for therapy, do something, anything, to raise your energy vibration. Please. We need everyone to do their part. Even if you think you’re totally good, you’re all better, there’s nothing to see here, you’ve done your work, even if you are totally terrified…I’m sure you are great the way you are and I know you are scared but there is always room for growth and there are some less terrifying options to choose from, so think of something you can do, and apply Jupiter time. Even if you don’t want to do your internal healing work to raise your energy vibration, you can still take part in the shift. Remember, tapping into source consciousness through methods like meditation and dream work allows you to access the unlimited knowledge base. From here, you can help humanity by finding answers to the problems we are currently facing. Even if you don’t really care about raising your energy vibration to make the world a better place, I bet the idea of tapping into an unlimited knowledge base to solve problems, make discoveries and see the future is at least somewhat appealing to you. In order to do this, you need to raise your energy vibration, at least temporarily. Do I have everyone’s attention now? Good. I’m going to give you lots of ideas so you can’t say that you don’t know what to do.
Nutrition.
Did you know that by simply choosing healthier, unprocessed organic food options, you can raise your energy vibration? Yep. If you don’t believe me, think about how you feel when you’ve been eating garbage food (e.g., after the holidays) versus how you feel after you eat nutrient-dense meals made with lots of fruits and vegetables. You are what you eat, right? Literally (Hawkins, 2002; McGinley, 2019).
Listen to music.
Listening to certain music can also raise (or lower) your energy vibration. Sound is a vibration, so it makes sense that it would interact with the energy vibration of your body. Remember our discussion on vibrational therapy and cats purring? Certain vibrations have the power to heal. I bet you already have some songs you like to listen to because they make you feel better. Now, that you know they are raising your energy vibration, you can listen to them deliberately with this intent. The Solfeggio frequencies have become popular recently for their use in raising energy vibration, balancing chakras, and physical and mental wellness. There are also some Hindu mantras you can listen to and chant with to raise your energy vibration. My favorite is the Gayatri Mantra, which is a dedication to the sun god. There are free versions online, or you can download this version on iTunes.
Confess your sins/shame.
We talked about this earlier under “What do to about shame.” Write down your shameful secrets or confess them to a trusted person. Doing so will reduce your shame and raise your energy vibration.
Visit an energy healer, Reiki practitioner, acupuncturist or chiropractor.
Energy healing and therapy are nice complimentary services, each serving to release different aspects of the pain and traumas we’ve experienced. For those of you who are unable or unwilling to go to therapy, I’d highly recommend working with an energy healer to alleviate some of your symptoms and move some of the trauma energy out of your body. I’ve included links for several healers I highly recommend, some even offer online services.
Renée Vidal: offers online services.
Shelby Rose: offers online services.
Dana Aschoff: offers primarily in-person services. Located in the Minneapolis, Minnesota area.
Begin a meditation practice.
There are a lot of meditation resources on the internet. Try a few out and see what works for you.
I offer a free, 10-minute energy clearing meditation here.
Begin a journaling or introspective writing practice.
This will help you process how you are thinking, feeling and acting. It will also help you become consciously aware of how your old stories, beliefs, fears and wounds are currently impacting your life, often unconsciously.
Start by taking a few notes each time you feel lots of emotion, get stuck in a thought loop or do something that you wish you wouldn’t have done.
What was happening? What did you feel in your body? What emotions did you feel? What went through your mind? What memories popped in? What did you do? What might all this be about? Where does it come from? How can you use this knowledge to help you?
Do some inner child healing work.
The inner child and teen aspects of us are often responsible for causing issues in our lives because they are holding onto unconscious wounds, fears, beliefs and stories. These wounds, fears, beliefs and stories can be very difficult to find using traditional methods (e.g., Cognitive Behavioral Therapy, introspective writing) because these primarily access the conscious parts of the mind. If you are able to access these younger aspects of yourself in your unconscious mind, using special methodology designed to tap into the unconscious, it becomes easier to uncover and heal the wounds, fears, beliefs and stories hiding in the shadows.
I have an excellent inner child and teen healing meditation journey here.
Begin a self-care practice.
Make time for yourself to do enjoyable, nurturing and restorative activities.
Some ideas: Read a novel, take a bath, get a massage, spend time with your friends, buy or make your favorite foods, call a good friend, do an art or craft project, go for a walk, spend time in nature, take a nap, sit in a sauna, float in the water, do absolutely nothing.
Work with crystals.
Crystals have a variety of properties, including the ability to raise energy vibration and promote physical and emotional healing. Each type of crystal has a unique set of properties. For example, selenite is a high vibrational crystal used to raise energy vibration, clear negative energy and clear the mind (Stokes, 2021). Agate is associated with Asclepius, the god of medicine, and is used for emotional and physical healing (Cunningham, 2004). If you are interested in learning more, I’ve included a couple of reference books below.
You can also buy agate jewelry, made by yours truly, here.
The Encyclopedia of Crystals by Judy Hall
The Ultimate Guide to Crystals & Stones: A Practical Path to Personal Power, Self-Development, and Healing by Uma Sibley
Learn to work with your dreams.
As we discussed, inventors, scientists, revolutionaries and healers throughout history have used dreams and dream-like states to tap into source consciousness in order to make important discoveries, develop theories, see the future and provide healing. Dreams are a largely untapped source of wisdom, advice and healing.
I offer a “Basics & Beyond” dream interpretation course, where you’ll learn how to access the source consciousness knowledge base through dreams to find healing, wisdom, advice, novel solutions and even get glimpses of the future. You can access this self-paced online dream interpretation course here.
Take an online course.
Shelby Rose offers some great classes that can help raise your energy vibration.
The Institute of Noetic Sciences has some wonderful offerings designed to raise your consciousness and develop extrasensory abilities.
The Aslan Institute offers online courses on shame, inner child healing, archetypes, death and aging that incorporate the evolution of consciousness framework.
Lean In, Make Bank is an excellent course by Tiffany McLain, designed to help therapists recognize their worth and begin charging accordingly. At its heart, it’s a course that teaches people to change their mindset and evolve their consciousness.
Money Mentality Makeover and Turning Shit Into Gold are advanced-level manifesting courses taught by Amanda Frances, designed to evolve consciousness and manifest money, relationships and pretty much anything else you’d like in life.
Listen to a personal growth podcast.
Podcasts are great because they allow you to multitask. You could even complete two, energy-raising activities at once: Listening to a personal growth podcast while making a nutritious meal!
Raise Your Vibration: Shelby Rose
Unlocking Us and Dare to Lead: Brené Brown
Read a book on personal growth or consciousness evolution.
Good books have the power to change us, and raise our energy vibration. Hawkins (2002) says that reading his book, Power vs Force, can raise someone’s energy vibration by 10 to the power of 35 points. That may sound like a convenient theory for him, but I think we’ve all had the experience of being different, better, as a result of what we’ve read in a book. For those who don’t like to read or don’t have the time, almost all books are available in audio format now. So, just like with podcasts, you can multitask your personal growth journey. Here are a few of my recommendations.
The Celestine Prophecy by James Redfield
The Big Leap by Gay Hendricks
Power vs Force: The Hidden Determinants of Human Behavior by David Hawkins
Destiny of Souls by Michael Newton
Women Who Run with the Wolves by Clarissa Pinkola Estes
Iron John by Robert Bly
Care of the Soul by Thomas Moore
Descent to the Goddess: A Way of Initiation for Women by Sylvia Brinton Perera
Man’s Search for Meaning by Viktor Frankl
The Book of Job: When Bad Things Happened to a Good Person by Harold S. Kushner
Living Beautifully with Uncertainty and Change by Pema Chödrön
The Will to Change: Men, Masculinity and Love by bell hooks
All About Love by bell hooks
Wired for Love: How Understanding Your Partner’s Brain and Attachment Style Can Help You Defuse Conflict and Build a Secure
Relationship by Stan Tatkin
The Highly Sensitive Person: How to Thrive When the World Overwhelms You by Elaine Aron
Adult Children of Emotionally Immature Parents by Lindsay Gibson
The Verbally Abusive Relationship by Patricia Evans
Toxic Parents: Overcoming Their Hurtful Legacy and Reclaiming Your Life by Susan Forward
Psychopath Free: Recovering From Emotionally Abusive Relationships with Narcissists, Sociopaths and Other Toxic People by Jackson MacKenzie
You Are the One You’ve Been Waiting for: Bringing Courageous Love to Intimate Relationships by Richard Schwartz
The Soul of Money by Lynne Twist
Mystical Dogs: Animals as Guides to Our Inner Life by Jean Houston
Supernormal: Science, Yoga, and the Evidence for Extraordinary Psychic Abilities by Dean Radin
Real Magic: Ancient Wisdom, Modern Science and a Guide to the Secret
Power of the Universe by Dean Radin
Sidewalk Oracles: Playing with Signs, Symbols, and Synchronicity in Everyday Life by Robert Moss
My Life with the Spirits: The Adventures of a Modern Magician by Lon Milo DuQuette
Join an environmental or social justice group and/or sign some petitions.
Don’t like what’s going on in this country? Want to see some changes? Join an environmental or social justice group and/or sign some petitions. It’s often free to do so. Even if you don’t have a lot of time to be involved with a group, by joining, you will have the opportunity to become apprised of important social and environmental issues. And, you’ll have the opportunity to make change simply by signing petitions, sending letters to Congress or donating small amounts of money to these causes, which usually only takes a few seconds. These groups use templates that make it really easy for you to simply type in your name and send a petition or letter along to the intended party. I’ll include some organizations I’d recommend checking out. Most are environmental advocacy groups because that’s one of my biggest passions, but you can do some searches online to find causes you are passionate about.
Stop your complicity in the exploitation of other human beings and the environment by choosing not to support the companies (and industries) that violate their rights.
If I had to guess, I’d say that about 99% of the products in our closets, cupboards, living rooms, refrigerators and garages are made (at least in part) by companies (and industries) that fall in this category. It’s nearly impossible to escape. We are dependent upon the continuation of slave and child labor as well as environmental exploitation and destruction, even though they’ve been outlawed or supposedly regulated in this country. But, we don’t have to be dependent and complicit participants. Each day, we make choices to support these companies and their exploitative practices by buying their products.
Choose differently. Find companies that are trying to do better and buy your products from them.
Stop participating in the continuation of forced obsolesce by continuing to upgrade your products, especially electronics.
Pay the extra money to have products repaired, rather than replacing them with brand-new products.
Buy used items to promote the practice of re-use and save money in the process.
Remember the law of supply and demand from economics class? We can extend that beyond product pricing to say that if there is no longer a demand for products that exploit people and the environment, companies will no longer produce them. If there is a demand for products and practices that support people and the environment, companies will begin to produce them.
The first step is to REDUCE your consumption and footprint. If you must consume and leave a footprint, then REUSE everything you can. And, if you can’t do either of those, as a last resort, RECYCLE. Recycling is better than using the landfill but it still requires additional energy and produces pollution, so always try to reduce and reuse first.
You can also help by sharing this manifesto on social media and with anyone you think it could help or would be interested in reading it.
We Have to Look
I know that no one wants to look at what’s lurking in the shadows within themselves and our culture, to face our painful pasts, to face the painful things we’ve done to others, to change our comfortable and convenient ways. And, I know that societal narratives; sociopolitical, cultural, economic and educational forces; our egos and even our own DNA, may be fighting growth and change with every step we take. We hate the idea of being vulnerable, addressing our problems, asking for help. We are terrified, so we don’t do it. Here’s the deal. We are ALL afraid of the dark. No one wants to go a therapist; no one wants to introspect; no one wants to peer into the shadows. Having courage means being afraid and doing things anyway. Take it from this hypocrite. It took me 34 years to face my ego fears, admit I needed help and finally start therapy—34 years! Then it took another two years before I was willing to do the really hard, painful, trauma-processing work. And, I know better. I know better than anyone how important therapy is, how well it works, how it has the power to change not only us as individuals but the world around us. Not only that, I know all about the ego’s defenses and how to overcome them. And, it still took a major act of courage for me to face my fears. It took the power of love. I hope the rest of you can draw upon the power of love, the love you have for other people, for animals, for the planet, for a cause, for yourself, to gain the courage you need to heal yourself and ultimately heal the world.
I Will Leave You with an Excerpt From the Great, Carl Sagan, and Pale Blue Dot (1994).
"Look again at that dot. That's here. That's home. That's us. On it everyone you love, everyone you know, everyone you ever heard of, every human being who ever was, lived out their lives. The aggregate of our joy and suffering, thousands of confident religions, ideologies, and economic doctrines, every hunter and forager, every hero and coward, every creator and destroyer of civilization, every king and peasant, every young couple in love, every mother and father, hopeful child, inventor and explorer, every teacher of morals, every corrupt politician, every "superstar," every "supreme leader," every saint and sinner in the history of our species lived there--on a mote of dust suspended in a sunbeam.
The Earth is a very small stage in a vast cosmic arena. Think of the rivers of blood spilled by all those generals and emperors so that, in glory and triumph, they could become the momentary masters of a fraction of a dot. Think of the endless cruelties visited by the inhabitants of one corner of this pixel on the scarcely distinguishable inhabitants of some other corner, how frequent their misunderstandings, how eager they are to kill one another, how fervent their hatreds.
Our posturings, our imagined self-importance, the delusion that we have some privileged position in the Universe, are challenged by this point of pale light. Our planet is a lonely speck in the great enveloping cosmic dark. In our obscurity, in all this vastness, there is no hint that help will come from elsewhere to save us from ourselves.
The Earth is the only world known so far to harbor life. There is nowhere else, at least in the near future, to which our species could migrate. Visit, yes. Settle, not yet. Like it or not, for the moment the Earth is where we make our stand.
It has been said that astronomy is a humbling and character-building experience. There is perhaps no better demonstration of the folly of human conceits than this distant image of our tiny world. To me, it underscores our responsibility to deal more kindly with one
another, and to preserve and cherish the pale blue dot, the only home we've ever known."
Expand the minds of others: Share this manifesto (social share links at the bottom).
References
American Psychiatric Association. (2019). APA Applauds Mental Health Funding in Federal Spending Bill [Press release]. Retrieved from https://www.psychiatry.org/newsroom/news-releases/apa-applauds-mental-health-funding-in-federal-spending-bill
Apostles’ Creed. (500 AD/2012). The Apostles’ Creed. In: Eternal Word Television Network.
Aron, E. N. (2016). The Highly Sensitive Person: How to Thrive When the World Overwhelms You. New York: Harmony Books.
Association of American Medical Colleges. (2008). Diversity in Medical Education: Facts & Figures 2008. Retrieved from Washington, D.C.: https://www.aamc.org/system/files/reports/1/diversityinmedicaleducation-factsandfigures2008.pdf
Baran, M. (2018, October 18). Why U.S. Workers Need to Step Up Their Vacation Game. Afar. Retrieved from https://www.afar.com/magazine/why-us-workers-need-to-step-up-their-vacation-game
Bardugo, L. (2017). The Shadow and Bone Trilogy Boxed Set: Shadow and Bone, Siege and Storm, Ruin and Rising New York: Square Fish.
Beck, A., T., Rush, A. J., Shaw, B. F., & Emery, G. (1987). Cognitive Therapy of Depression. New York: Guilford Press.
Benecchi, L. (2021). Recidivism Imprisons American Progress. harvard Political Review. Retrieved fromhttps://harvardpolitics.com/recidivism-american-progress/
Bick, A., Brüggemann, B., & Fuchs-Schündeln, N. (2016). Hours worked in Europe and the US: New data, new answers. Institute for the Study of Labor, 10179, 1-44.
Bluth, K., Gaylord, S., Nguyen, K., Bunevicius, A., & Girdler, S. (2015). Mindfulness-based Stress Reduction as a Promising Intervention for Amelioration of Premenstrual Dysphoric Disorder Symptoms. Mindfulness, 6, 1292-1302. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4651211/
Boissoneault, L. (2019, May 21, 2019). The Medieval Practices That Reshamed Europe’s Fish. The Atlantic. Retrieved from https://www.theatlantic.com/science/archive/2019/05/medieval-people-were-already-ruining-fish/589837/
Bourne, J. (2008). Slavery in the United States. In R. Whaples (Ed.), (March 26 ed.). Retrieved from http://eh.net/encyclopedia/slavery-in-the-united-states/
Bradley, R., Greene, J., Russ, E., Dutra, L., & Westen, D. (2005). A multidimensional meta-analysis of psychotherapy for PTSD. American Journal of Psychiatry, 162(2), 214–227. Retrieved from https://ajp.psychiatryonline.org/doi/pdf/10.1176/appi.ajp.162.2.214
Cahill, S. P., Foa, E. B., Hembree, E. A., Marshall, R. D., & Nacash, N. (2006). Dissemination of exposure therapy in the treatment of PTSD. Journal of Traumatic Stress, 19(5), 597-610. Retrieved from https://www.med.upenn.edu/ctsa/assets/user-content/documents/CahillFoa_Dissemination_2006.pdf
Cambray, J. (2009). Synchronicity: Nature and Psyche in an Interconnected Universe. College Station: Texas A&M University Press.
Centers for Disease Control and Prevention. Violence Prevention: Risk and Protective Factors. Adverse Childhood Experiences. Retrieved from https://www.cdc.gov/violenceprevention/aces/riskprotectivefactors.html
Claes, L., & Willie, B. (2007). The enhancement of bone regeneration by ultrasound. Progress in Biophysics and Molecular Biology, 93(1-3), 384-398. Retrieved from https://reader.elsevier.com/reader/sd/pii/S0079610706001027?token=83F8A3230020D10B180E644968B21821E29D775B1E35D99945D779D9AA8EECA59AA99379277CFEA3595AFB8079F3085A&originRegion=us-east-1&originCreation=20220101174354
Cohen, R. (2021, December 13). Across the World, COVID Anxiety and Depression Take Hold. New York Times. Retrieved from https://www.nytimes.com/2021/12/13/world/europe/covid-anxiety-depression-omicron.html
Collins, J. (2001). Good to Great: Why Some Companies Make the Leap and Others Don’t. New York: HarperBusiness.
Crittenden, A. (2006). How Mothers’ Work Was “Disappeared”: The Invention of the Unproductive Housewife. In A. S. Wharton (Ed.), Working in America: Continuity, Conflict, and Change (3rd ed., pp. 18-31). New York: McGraw-Hill.
Cunningham, S. (2004). Wicca: A Guide for the Solitary Practitioner. Woodbury, Minnesota: Llewellyn Publications.
Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M., Muller, D., Santorelli, S. F., . . . Sheridan, J. F. (2003). Alterations in Brain and Immune Function Produced by Mindfulness Meditation. Psychosomatic Medicine, 65(4), 564-570. Retrieved from https://journals.lww.com/psychosomaticmedicine/Abstract/2003/07000/Alterations_in_Brain_and_Immune_Function_Produced.14.aspx
DeRubeis, R. J., Hollon, S. D., Amsterdam, J. D., Shelton, R. C., Young, P. R., Salomon, R. M., & Gallop, R. (2005). Cognitive therapy vs medications in the treatment of moderate to severe depression. Archives of General Psychiatry, 62(4), 409-416. Retrieved from https://jamanetwork.com/journals/jamapsychiatry/fullarticle/208460
Dowling, S. (2018, July 25, 2018). The complicated truth about a cat’s purr. BBC Future. Retrieved from https://www.bbc.com/future/article/20180724-the-complicated-truth-about-a-cats-purr
Eisenstadt v. Baird. (1972). Unmarried Couples have the right to use contraception, based on the Equal Protection Clause of the Fourteenth Amendment and the more nebulous constitutional right to privacy. U.S. Supreme Court, 405(U.S. 438).
English, J. (2020). Why Do Habitual Offenders Keep Reoffending? (Pt 1). The Kronzek Firm, PLC. Retrieved from https://aggressivecriminaldefense.com/why-do-habitual-offenders-keep-reoffending-pt-1.html
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., . . . Marks, J. S. (1998). Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventative Medicine, 14(4), 245-258. Retrieved from https://www.ajpmonline.org/action/showPdf?pii=S0749-3797%2898%2900017-8
Foa, E. B., Keane, T. J., & Friedman, M. J. (2000). Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress Studies. New York: Guilford Press.
Greene, B. (2004). The Fabric of the Cosmos: Space, Time and the Texture of Reality. New York, New York: Vintage Books.
Groysberg, B., & Abrahams, R. (2020). What the Stockdale Paradox Tells Us About Crisis Leadership. Harvard Business School: Working Knowledge. Retrieved from https://hbswk.hbs.edu/item/what-the-stockdale-paradox-tells-us-about-crisis-leadership
Harvey, A. G., Bryant, R. A., & Tarrier, N. (2003). Cognitive behaviour therapy for posttraumatic stress disorder. Clinical Psychology Review, 23(3). Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0272735803000357?via%3Dihub
Hawkins, D. R. (2002). Power Vs. Force: The Hidden Determinants of Human Behavior. Carlsbad, California: Hay House Inc.
He, S., Zhao, W., Zhang, L., Mi, L., Du, G., Sun, C., & X., S. (2017). Low-frequency vibration treatment of bone marrow stromal cells induces bone repair in vivo. Iranian Journal of Basic Medical Sciences, 20(1), 23-28. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5243970/pdf/IJBMS-20-23.pdf
Hendricks, G. (2009). The Big Leap: Conquer Your Hidden Fear and Take Life to the Next Level. New York: HarperOne.
Hicks, E., & Hicks, J. (2006). The Law of Attraction: The Basics of the Teachings of Abraham. Carlsbad, CA: Hay House, Inc.
Hofmann, S. G., Moscovitch, D. A., Kim, H.-J., & Taylor, A. N. (2004). Changes in self-perception during treatment of social phobia. Journal of Consulting and Clinical Psychology, 72, 588–596. Retrieved from https://psycnet.apa.org/record/2004-16970-004
Hollis, J. (2013). Hauntings: Dispelling the Ghosts Who Run Our Lives. Asheville, North Carolina: Chiron Publications.
Hopwood, A. Jung’s Model of the Psyche. Retrieved from https://www.thesap.org.uk/articles-on-jungian-psychology-2/carl-gustav-jung/jungs-model-psyche/
Huddleston, C. (2019). Survey: 69% of Americans Have Less Than $1,000 in Savings. Retrieved from https://www.gobankingrates.com/banking/savings-account/americans-have-less-than-1000-in-savings/
Hülsheger, U. R., Feinholdt, A., & Nübold, A. (2015). A low-dose mindfulness intervention and recovery from work: Effects on psychological detachment, sleep quality, and sleep duration. Journal of Occupational and Organizational Psychology, 88(3). Retrieved from https://bpspsychub.onlinelibrary.wiley.com/doi/abs/10.1111/joop.12115
Hung, W. (2004, January 15). [American Idol Song]. Retrieved from https://www.youtube.com/watch?v=9RrLQUN8UJg
Huseyin, R. (2016). David Hawkins’ Map of Consciousness – Crazy, or Crazy Insightful? Retrieved from https://www.artofwellbeing.com/2016/11/08/mapofconsciousness/
Jefferson Airplane. (1966). White Rabbit. On Surrealistic Pillow. Hollywood, California: RCA Victor.
Jones, C. (1958). A Review of the Air Pollution Research Program of the Smoke and Fumes Committee of the American Petroleum Institute. Journal of the Air Pollution Control Association, 8(3), 268-272. Retrieved from https://www.documentcloud.org/documents/2827789-1958-Charles-Jones-Smoke-and-Fumes-Committee-of.html#document/p1/a366549
Kahneman, D., & Deaton, A. (2010). High income improves evaluation of life but not emotional well-being. Proceedings of the National Academy of Sciences of the United States of America, 107(38), 16489-16493. Retrieved from https://www.pnas.org/content/pnas/107/38/16489.full.pdf
Kim, A. (2019, August 19). A record 768 million US vacation days went to waste last year, a study says. CNN Travel. Retrieved from https://www.cnn.com/travel/article/unused-vacation-days-trnd/index.html
Klott, J. (2011). Motivational Interviewing for Mental Health Disorders. Training CD. Honolulu, HI: PESI: Premier Education Solutions.
Kopp, S. B. (1972). If You Meet the Buddha on the Road, Kill Him: The Pilgrimage of Psychotherapy Patients. Palo Alto, California: Science and Behavior Books, Inc.
Kretchmer, Z. A. (2018, December 6). [Personal Communication: Delighted or Contented?].
Lau, E., Al-Dujaili, S., Guenther, A., D., L., L., W., & You, L. (2010). Effect of low-magnitude, high-frequency vibration on osteocytes in the regulation of osteoclasts. Bone, 46(6), 1508-1515. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S8756328210004928?via%3Dihub
Linehan, M. (2017). Marsha Linehan: How She Learned Radical Acceptance [YouTube]. Retrieved from https://www.youtube.com/watch?v=OTG7YEWkJFI&feature=youtu.be
Luborsky, L., Rosenthal, R., Diguer, L., Andrusyna, T. P., Berman, J. S., Levitt, J. T., . . . Krause, E. D. (2002). The dodo bird verdict is alive and well--mostly. Clinical Psychology: Science and Practice, 9(1), 2-12. Retrieved from https://doi.apa.org/doiLanding?doi=10.1093%2Fclipsy.9.1.2
Matthews, G. (2007). The Impact of Commitment, Accountability, and Written Goals on Goal Achievement. Paper presented at the 87th Convention of the Western Psychological Association, Vancouver, British Columbia, Canada.
McGinley, K. (2019). How to Raise Your Emotional & Spiritual Vibration. Chopra. Retrieved from https://chopra.com/articles/a-complete-guide-to-raise-your-vibration
McGreal, C. (2021, June 30). Big oil and gas kept a dirty secret for decades. Now they may pay the price. The Guardian. Retrieved from https://www.theguardian.com/environment/2021/jun/30/climate-crimes-oil-and-gas-environment
Monson, C. M., Schnurr, P. P., Resick, P. A., Friedman, M. J., Young-Xu, Y., & Stevens, S. P. (2006). Cognitive processing therapy for veterans with military-related posttraumatic stress disorder. Journal of Consulting and Clinical Psychology, 74(5), 898–907. Retrieved from https://cptforptsd.com/wp-content/uploads/2016/05/Monson_JCCP_2006_898.pdf
Moore, R. D., & Eick, D. (Producer). (2004). Battlestar Galactica.
Moss, R. (2009a). The Secret History of Dreaming. Novato, California: New World Library.
(2009b, March 13, 2009). The Secret History of Dreaming with Robert Moss [Retrieved from https://shrinkrapradio.com/199-the-secret-history-of-dreaming-with-robert-moss/
Moss, R. (2015). Sidewalk Oracles: Playing with Signs, Symbols, and Synchronicity in Everyday Life. Novato, CA: New World Library.
New International Version. (1978/2011). Deuteronomy 5:9. Retrieved from https://www.biblegateway.com/verse/en/Deuteronomy%205%3A9
Newberg, A. B., Wintering, N., Khalsa, D. S., Roggenkamp, H., & Waldman, M. R. (2010). Meditation effects on cognitive function and cerebral blood flow in subjects with memory loss: A preliminary study. Journal of Alzheimer’s Disease, 20, 517–526. Retrieved from https://pubmed.ncbi.nlm.nih.gov/20164557/
Norcross, J. C., & Kuhle, B. X. (2011, Summer). New Probabilities of Admission Into Graduate Psychology Programs.Eye on Psi Chi, pp. 21-22. Retrieved from https://psychology.oglethorpe.edu/files/2015/07/Psi_Chi_magazine_2011_gradadmissions.pdf
Ogren, J. (2019). Psychological Shamanism. In: Institute of Noetic Sciences.
Olson-Raymer, G. (2014). The Europeans: Why They Left and Why It Matters. Retrieved from http://gorhistory.com/hist110/expl.html
Omar, H., Shen, G., Jones, A. S., Zoellner, H., Petocz, P., & Darendeliler, M. A. (2008). Effect of low magnitude and high frequency mechanical stimuli on defects healing in cranial bones. Journal of Oral and Maxillofacial Surgery, 66(6), 1104-1111. Retrieved from https://www.joms.org/article/S0278-2391(08)00112-2/fulltext
Payne, R. (2006). Planet Earth: The Future. Great Britain: British Broadcasting Company.
PayScale. Salary Data & Career Research Center (United States). Retrieved from https://www.payscale.com/research/US/
PBS (Producer). Indentured Servants In The U.S. History Detectives Retrieved from https://www.pbs.org/opb/historydetectives/feature/indentured-servants-in-the-us/
Planck, M. (1931, January 25). The Observer.
Plumer, B., & Fountain, H. (2021, August 9, 2021). A Hotter Future Is Certain, Climate Panel Warns. but How Hot Is Up to Us. The New York Times. Retrieved from https://www.nytimes.com/2021/08/09/climate/climate-change-report-ipcc-un.html
Radin, D. (2013). Supernormal: Science, Yoga, and the Evidence for Extraordinary Psychic Abilities. New York: Deepak Chopra Books.
Radin, D. (2018). Real Magic: Ancient Wisdom, Modern Science, and a Guide to the Secret Power of the Universe. New York: Harmony Books.
Razon, S., Pickard, K. B., McCown, D. A., & Reed, M. A. (2017). Effects of Meditation on Heart Rate and Blood Pressure: A Mindfulness-based Study. Internationa Journal of Exercise Science, 9(6).
Redfield, J. (1993). The Celestine Prophecy: An Adventure. New York: Time Warner Books.
Resick, P. A., Monson, C. M., & Chard, K. M. (2008). Cognitive Processing Therapy: Veteran/military version. Washington, D.C.: Department of Veterans’ Affairs.
Resick, P. A., Nishith, P., Weaver, T. L., Astin, M. C., & Feuer, C. A. (2002). A comparison of cognitive processing therapy, prolonged exposure and a waiting condition for the treatment of posttraumatic stress disorder in female rape victims. Journal of Consulting and Clinical Psychology, 70(4), 867–879. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2977927/pdf/nihms247366.pdf
Resick, P. A., & Schnicke, M. K. (1992). Cognitive processing therapy for sexual assault victims. Journal of Consulting and Clinical Psychology, 60(5), 748–756.
Resick, P. A., & Schnicke, M. K. (1993). Cognitive processing therapy for rape victims: A treatment manual. Newbury Park, CA: Sage Publications.
Resignation, W.-G. Great Resignation. Retrieved from https://en.wikipedia.org/wiki/Great_Resignation. Retrieved December 17, 2021, from Wikipedia https://en.wikipedia.org/wiki/Great_Resignation
Rogers, E. M. (1962). Diffusion of innovations (1st ed.). New York: Free Press of Glencoe.
A. Malone (Director). (1980, November 30, 1980). The Edge of Forever [Television series episode]. In Sagan, C. (Executive producer), Cosmos: PBS.
Sagan, C. (1994). Pale Blue Dot: A Vision of the Human Future in Space. New York: Random House.
Scientific American. (2006, April 3). Why do cats purr? Scientific American. Retrieved from https://www.scientificamerican.com/article/why-do-cats-purr/
Selimbasic, Z., Sinanovic, O., & Avdibegovic, E. (2012). Psychosocial Problems Among Children of Parents with Posttraumatic Stress Disorder. Medical Archives, 66(5), 304-308. Retrieved from https://www.bibliomed.org/mnsfulltext/10/10-1348126424.pdf?1640906255
Sheldrake, R. Morphic Resonance and Morphic Fields: An Introduction. Retrieved from https://www.sheldrake.org/research/morphic-resonance/introduction
Shneiderman, D., Sanders, D., & March, K. (2017). Ancient Egyptian vs. Mayan Culture. Classroom. Retrieved from https://classroom.synonym.com/tools-used-artists-ancient-egypt-15484.html
Sinek, S. (2009). Start with Why: How Great Leaders Inspire Everyone to Take Action. New York: Portfolio.
Singer, J. (1972). Boundaries of the Soul: The Practice of Jung’s Psychology. Garden City, New York: Anchor Press-Doubleday.
Smith, P. (2017). The Hidden Prison Crisis: How Homelessness Causes A Cycle Of Reoffending. BuzzFeed News. Retrieved from https://www.buzzfeed.com/patricksmith/the-hidden-prison-crisis-how-homelessness-causes-a-cycle-of
Snyder, J., Gewirtz, A., Schrepferman, L., Gird, S. R., Quattlebaum, J., Pauldine, M. R., . . . Hayes, C. (2016). Parent-Child Relationship Quality and Family Transmission of Parent Posttraumatic Stress Disorder Symptoms and Child Externalizing and Internalizing Symptoms Following Fathers’ Combat-Trauma Exposure. Developmental Psychopathology, 28(4 Pt 1), 947-969. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5113136/pdf/nihms826555.pdf
Steele, M. (2020, April 20). [Mentoring Session: COVID-19 Dicussion].
Stokes, V. (2021). Selenite Crystal: Healing Properties, Lore, And How to Use This High Vibration Stone. Healthline. Retrieved from https://www.healthline.com/health/mind-body/selenite-properties
Supran, G. Presentation: Assessing ExxonMobil’s Climate Change Communications: Have communications about climate change by ExxonMobil and other fossil fuel companies misled customers, shareholders, or the public?https://www.europarl.europa.eu/cmsdata/162144/Presentation%20Geoffrey%20Supran.pdf
Supran, G., & Oreskes, N. (2017). Assessing ExxonMobil’s climate change communications (1977–2014). Environmental Research Letters, 12, 1-18. Retrieved from https://iopscience.iop.org/article/10.1088/1748-9326/aa815f/pdf
Supran, G., & Oreskes, N. (2020). Addendum to ‘Assessing ExxonMobil’s climate change communications (1977–2014)’ Supran and Oreskes (2017 Environ. Res. Lett. 12 084019). Environmental Research Letters, 15, 1-18. Retrieved from https://iopscience.iop.org/article/10.1088/1748-9326/aa815f/pdf
Talbot, M. (1988). Beyond the Quantum. New York, New York: Bantam Books.
The Eagles. (1977). Hotel California. On Hotel California. Los Angeles, CA: Asylum.
Timperley, J. (2021, October 21). The fight to end fossil-fuel subsudies: Why is it so hard to stop governments propping up of the coal, oil and gas industries? Nature, 598, 403-405. Retrieved from https://media.nature.com/original/magazine-assets/d41586-021-02847-2/d41586-021-02847-2.pdf
Trismegistus, H. The Emerald Tablet of Hermes. In.
Turakitwanakan, W., Mekseepralard, C., & Busarakumtragul, P. (2013). Effects of Mindfulness Meditation on Serum Cortisol of Medical Students. JOurnal of the Medical Association of Thailand, 96. Retrieved from https://pubmed.ncbi.nlm.nih.gov/23724462/
U.S. Department of Housing and Urban Development. (2016). Discrimination Against Families with Children in Rental Housing Markets: Findings of the Pilot Study. Retrieved from https://www.huduser.gov/portal/sites/default/files/pdf/HDSFamiliesFinalReport.pdf
von Muggenthaler, E. (2001). The felid purr: A healing mechanism? The Journal of the Acoustical Society of America, 110(5), 2666. Retrieved from https://www.researchgate.net/publication/272259095_The_felid_purr_A_healing_mechanism
Wampold, B. E., Minami, T., Baskin, T. W., & Tierney, S. C. (2002). A meta-(re)analysis of the effects of cognitive therapy versus ‘other therapies’ for depression. Journal of Affective Disorders, 68(2-3), 159–165. Retrieved from https://www.sciencedirect.com/science/article/abs/pii/S0165032700002871?via%3Dihub
Wikipedia-Ableism. Ableism. Retrieved from https://en.wikipedia.org/wiki/Ableism. Retrieved December 6, 2021 https://en.wikipedia.org/wiki/Ableism
Wikipedia-Annual Leave. List of minimum annual leave by country. Retrieved from https://en.wikipedia.org/wiki/List_of_minimum_annual_leave_by_country. Retrieved January 20, 2022 https://en.wikipedia.org/wiki/List_of_minimum_annual_leave_by_country
Wikipedia-Dodo Bird Verdict. Dodo Bird Verdict. Retrieved from https://en.wikipedia.org/wiki/Dodo_bird_verdict. Retrieved December 11, 2021 https://en.wikipedia.org/wiki/Dodo_bird_verdict
Wikipedia-Internet Troll. Internet Troll. Retrieved from https://en.wikipedia.org/wiki/Internet_troll. Retrieved January 4, 2022 https://en.wikipedia.org/wiki/Internet_troll
Wikipedia-Quantum Enganglement. Quantum Enganglement. Retrieved from https://en.wikipedia.org/wiki/Quantum_entanglement. from Wikipedia https://en.wikipedia.org/wiki/Quantum_entanglement
Wikipedia-Stockdale. James Stockdale. Retrieved from https://en.wikipedia.org/wiki/James_Stockdale. Retrieved December 18, 2021 https://en.wikipedia.org/wiki/James_Stockdale
Wikipedia-Turning…Cheek. Turning the Other Cheek. Retrieved from https://en.wikipedia.org/wiki/Turning_the_other_cheek. Retrieved November 11, 2021 https://en.wikipedia.org/wiki/Turning_the_other_cheek
Williamson, M. (2002). Everyday Grace: Having Hope, Finding Forgiveness and Making Miracles. New York: Riverhead Books.
Wilson, E. O. (2006). Planet Earth: The Future. Great Britain: British Broadcasting Company.
Worl-A-Girl. (1993). Jamaican Bobsledding Chant. Cool Runnings.
Youssef, N., A., Lockwood, L., Su, S., Hao, G., & Rutten, B. P. F. (2018). The Effects of Trauma, with or without PTSD, on the Transgenerational DNA Methylation Alterations in Human Offsprings. Brain Sciences, 8(83), 1-7. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5977074/pdf/brainsci-08-00083.pdf
Zimmerman, M. (1986). Neurophysiology of Sensory Systems, Robert F. Schmidt Ed., Fundamentals of Sensory Physiology. . In R. F. Schmidt (Ed.), Fundamentals of Sensory Physiology. Berlin.: Springer-Verlag.
Extracting Wisdom From COVID-19 Sleep Disturbances
Coronavirus is affecting our health in more ways than direct viral infection. Twenty-two percent of us are reporting trouble sleeping, with Gen Xers being the most notably affected (Sleep Help, 2020).
We are scared, our lives have been completely upended, we no longer have our regular routines to distract and anesthetize us, and, even if we are COVID-19 free, we are developing a nasty case of cabin fever. Further, without the distractions of our normal routines and with the stirring of deep emotions within us, we are coming face to face with our own demons (and the demons of our household members). It’s no wonder we are having trouble sleeping.
Coronavirus is affecting our health in more ways than direct viral infection. Twenty-two percent of us are reporting trouble sleeping, with Gen Xers being the most notably affected (Sleep Help, 2020).
We are scared, our lives have been completely upended, we no longer have our regular routines to distract and anesthetize us, and, even if we are COVID-19 free, we are developing a nasty case of cabin fever. Further, without the distractions of our normal routines and with the stirring of deep emotions within us, we are coming face to face with our own demons (and the demons of our household members). It’s no wonder we are having trouble sleeping.
Not only are we having trouble sleeping, anecdotal evidence suggests that we are dreaming less and when we do dream, our dreams tend to be more vivid and disturbing. Why is this?
When we experience traumatic or very stressful events, our psyche often blocks not only memories of the trauma but memories of our dreams, so we aren’t disturbed by them. If we do dream and are having disturbing dreams, as much as we may not like them, they are showing up for a reason. This is our psyche’s way of saying that something needs our attention. Like painful or traumatic events, dreams won’t go away simply by ignoring them. Further, the reality we are living in right now is essentially a bad dream. It’s as if the dream world and the physical world have been transposed. This may account for why we are not remembering our night dreams; that is, we are living them during the day (Steele, 2020).
What can you do about insomnia? Believe it or not, there is wisdom in insomnia. Some say that during this time, the veil between the worlds, the spirit world and earthly world, is thinnest, so messages from the spirit world are able to reach us (Andrews, 1993). Scientists, inventors, and revolutionaries have used insomnia, dreams and dreamlike states for millennia to develop theories, invent new technology, and see the future (e.g., Albert Einstein, Harriet Tubman, Alexander the Great). John Lennon said, “The best songs are the ones that come to you in the middle of the night and you have to get up and write them down, so you can go back to sleep,” (Moss, 2009). Your brain is incredibly efficient and rarely engages in mental processes unless they are useful, so trust that it’s trying to help you, trying to work something out. And, it doesn’t take a Ph.D. in psychology to recognize that there are some major things our brains are trying to work out right now, both individually and as a collective.
Rather than viewing insomnia as the bane of your existence and fighting it, view it as helpful and literally ask, “Insomnia, why are you here?” Use a journal or audio app on your phone:
1. Write or say anything that comes to mind, no matter how relevant it seems (Freud called this free association). If it’s popping into your mind, it’s popping in for a reason.
2. If something resonates or rings true, you’ve likely hit pay dirt and uncovered some deep wisdom.
3. Turn that wisdom into an axiom, affirmation, or warning and apply it to your life.
What can you do about disturbing dreams? As counterintuitive as it seems, as with insomnia, I would also recommend embracing the message of disturbing dreams by asking why they are here. Next, spend some time being present to and understanding your feelings and thoughts surrounding the dream:
1. What feelings/thoughts/bodily sensations are showing up for you?
2. What’s this about?
3. What does it all mean to you?
4. Write or say anything that comes to mind, no matter how relevant it seems.
5. If something resonates or rings true, note that.
6. Turn that wisdom into an axiom, affirmation, or warning and apply it to your life.
If you feel overwhelmed, it’s okay to take a break and try some of the strategies I’ve discussed below. Even if we hate what we feel and find it overwhelming, know that our systems are wired to handle the emotional energy we produce.
1. Reach out to a loved one for support.
2. Do something kind for yourself (e.g., treat yourself to your favorite show, book, food; spend time in nature).
3. Use a relaxation technique, like diaphragmatic breathing. https://www.healthline.com/health/diaphragmatic-breathing#steps-to-do
4. Try a guided meditation.
https://www.youtube.com/watch?v=a_O1R9T0Uu4
5. If you don’t feel like you can manage what’s showing up, find a therapist or healer. This is what we are here for.
6. If you’d like more help working with your dreams or insomnia, you can reach me through my website to schedule a consultation for therapy, a dream interpretation session, or preregister for my online course, “Dream Interpretation: The Basics and BEYOND.”
https://www.briannamannphd.com
References
Andrews, T. (1993). Animal Speak: The Spiritual and Magical Powers of Creatures Great and Small. Woodbury, Minnesota: Llewelyn Publications.
Moss, R. (2009). The Secret History of Dreaming. Novato, California: New World Library.
Sleep Help. (2020). The Effects of COVID-19 on Sleep: Exploring How the Coronavirus Impacts People’s Sleep Habits. Retrieved from https://www.sleephelp.org/covid-19-impact-on-sleep/?mod=article_inline
Steele, M. (2020, March 23, 2020). [Mentoring Session: March 23rd, 2020].
Why Mental Health Providers Should Think Twice Before Credentialing with Health Insurance: Ramifications for Therapists, Clients and the Field of Mental Health
An excerpt from this article was published on Hey Tiffany: https://www.heytiffany.com/problems-with-insurance-for-therapists-in-private-practice/
Reasons Providers Credential with Health Insurance
The reasons why providers credential with the insurance companies are reasonable. First, credentialing with health insurance is the status quo; it’s what everyone does. Second, credentialing is one way to ensure that providers have a steady referral stream without having to do a lot of outside marketing. Third, credentialing with insurance allows providers to provide access to care to a wide demographic of individuals, including those who might not be able to afford therapy out-of-pocket. Fourth, the benefits of credentialing compensate for skills deficits and fears most mental health providers have: A) Few therapists know how to market or how to run a small business, because these are not skills taught in graduate school. Therapists have little confidence in succeeding in marketing and business management. B) In fact, these are skills that are discouraged both explicitly and implicitly throughout therapists’ training; marketing and running a business that makes money are seen as “bad”, and running a charitable practice with “affordable” fees and pro bono work is seen as “good”. C) Many therapists are incredulous that potential clients, who have already purchased a health insurance plan, will be willing to pay out-of-pocket for an additional service. D) Scarcity motivates providers, especially those just starting out, to accept whatever they can get; some money is better than no money. I’m certainly familiar with these rationale and fears, and I don’t fault anyone for utilizing these rationale and trying to mitigate their fears. I do, however, think it’s time to critically examine the ramifications of credentialing with insurance for mental health providers, clients, and the field of mental health for the purpose of making an informed decision about whether to continue this practice.
An excerpt from this article was published on Hey Tiffany: https://www.heytiffany.com/problems-with-insurance-for-therapists-in-private-practice/
Brianna D. Mann, Ph.D.
Reasons Providers Credential with Health Insurance
The reasons why providers credential with the insurance companies are reasonable. First, credentialing with health insurance is the status quo; it’s what everyone does. Second, credentialing is one way to ensure that providers have a steady referral stream without having to do a lot of outside marketing. Third, credentialing with insurance allows providers to provide access to care to a wide demographic of individuals, including those who might not be able to afford therapy out-of-pocket. Fourth, the benefits of credentialing compensate for skills deficits and fears most mental health providers have: A) Few therapists know how to market or how to run a small business, because these are not skills taught in graduate school. Therapists have little confidence in succeeding in marketing and business management. B) In fact, these are skills that are discouraged both explicitly and implicitly throughout therapists’ training; marketing and running a business that makes money are seen as “bad”, and running a charitable practice with “affordable” fees and pro bono work is seen as “good”. C) Many therapists are incredulous that potential clients, who have already purchased a health insurance plan, will be willing to pay out-of-pocket for an additional service. D) Scarcity motivates providers, especially those just starting out, to accept whatever they can get; some money is better than no money. I’m certainly familiar with these rationale and fears, and I don’t fault anyone for utilizing these rationale and trying to mitigate their fears. I do, however, think it’s time to critically examine the ramifications of credentialing with insurance for mental health providers, clients, and the field of mental health for the purpose of making an informed decision about whether to continue this practice.
Reason for Source Anonymity
To gather information for this article, I conducted a literature review and interviewed healthcare professionals. One provision of the health insurance contracts states that credentialed providers are not allowed to discuss the specifics of their contracts, and if they do discuss these specifics, they jeopardize their contracts. As such, many of the healthcare professionals I spoke with required anonymity as a condition of their interview; I am respecting this by not including their names. A discussion of the gag order placed by insurance companies on providers, prohibiting discussion of contract specifics is another article entirely. I point it out briefly to encourage critical thinking regarding the motivation for a gag order. Why would someone in power prohibit someone they have power over from a Constitutional right, freedom of speech? If you don’t know yet, maybe you’ll get a better idea as you read this article. At any rate, I appreciate my sources’ bravery in being willing to share anything at all with me.
I. The Business of Healthcare Has Turned Healthcare into a Business, Not Healthcare
A. Deregulation of Healthcare
1. Conflict of Interest
In 1983, something happened that would change the landscape of healthcare in America forever: The Reagan Administration deregulated healthcare. Specifically, this deregulation changed how providers were reimbursed for healthcare delivery costs. Previously, third-party reimbursement for healthcare to providers and larger entities, like hospitals, utilized a relative cost metric: Reimbursement rates were based upon the providers’ costs to provide the service along with a bit more to provide profit, which seems logical, linking reimbursement amount with actual service cost. With the changes to the law, the insurers changed their reimbursement metric from a relative rate to a fixed rate for each service, irrespective of true cost. If a service cost $100 to administer, the provider would no longer receive $100 plus profit, they would receive a fixed rate predetermined by the third-party payer. And, if the fixed rate was lower, for example, $80, the provider lost money. Now, rather than operating according to best practices and being reimbursed for the costs of operating according to those practices, providers were motivated to avoid a loss, and a conflict of interest developed: Operate according to best practices and potentially lose money or cut costs and operate as well as you can within those cost constraints. The change in reimbursement metric turned healthcare from a service industry into a business, and significantly increased third-party payers’ profit margins. Not only did reimbursement metrics change, many aspects of healthcare became for-profit, catering to investors rather than consumers (Frakt, 2018).
2. Power Differential
If a conflict of interest develops between profit and best practices, there would need to be a regulatory system to ensure that consumers aren’t harmed by such a conflict. But, in order for such a system to function, several conditions would need to be met. First, consumers would need to be aware that a conflict of interest with the potential to cause harm exists. And, I’m not entirely sure that most consumers are aware of how healthcare deregulation in the 1980’s has affected them. Second, someone would need to draw attention to the conflict of interest and ask for change. Third, that someone’s voice would need to be loud enough for someone else to take action. Whose voice is typically louder: the average American consumer or a multibillion dollar industry? Fourth, a mechanism would need to exist for holding an industry or company accountable. Under the Obama administration, there was a cabinet position for consumer protection; the funding for that position has since been eliminated (Grunwald, 2018). Fifth, even if the industry or company is held accountable for a specific incident, how likely is it that large scale changes will be made? Further, what is the likelihood that all of these conditions will be met? And, what typically happens when powerful, wealthy individuals or entities get in trouble? The problem here is a huge power differential between the average American consumer and the health insurance industry; this power differential renders consumers defenseless to protect themselves and ask for change.
3. The Goal of Health Insurance is Not to Help You, It’s to Make Money
a) An “Ingenious” Formula with a Low ROI for Consumers
The health insurance industry’s goal is not to help consumers, it is to make money. I don’t think that’s really a secret. That’s capitalism. But, it’s important for consumers to remember this fact when they are spending five figures on a policy to cover their healthcare expenses. What consumers also need to remember is that the product they are buying has an incredibly low return on investment (ROI) and is designed for the purpose of having an incredibly low ROI; that’s called the insurance company’s profit margin.
Do you know how health insurance companies make money? It’s a pretty simple formula: Insurance costs to consumers > reimbursed health care expenses. On average, insurance companies need to collect more money in premiums than they pay out to consumers in health care expenses. It’s no secret that this is how this works, but for some reason most of us consumers have it in our heads that using insurance gets us a good deal on our healthcare. It doesn’t. In fact, insurance companies call consumers’ medical expenses their “medical loss ratio”; in other words, having to pay for the service consumers purchased from them is seen by insurance companies as a loss, not as providing a service. Their hope is that consumers won’t use their service, and if they do, it’s seen as a loss (Lazarus, 2017).
I know that many insurers file their taxes as non-profit entities, but consumers should know that “nonprofit” doesn’t mean a company doesn’t make any money. Non-profit status means that the company “…uses its surplus of the revenues to further achieve its ultimate objective, rather than distributing its income to the organization’s shareholders, leaders, or members” (Wikipedia). So, the insurance companies can make a profit, they just can’t distribute it to shareholders, rather, they must use it to achieve their “ultimate objective”. What is the “ultimate objective” of the health insurance companies: to minimize their “medical loss ratio”? I really don’t know; that would be an important question to answer. A very curious fact is that the non-profit health insurance companies’ CEOs sure seem to make a lot of money. According to a Minnesota Star Tribune article, the state-level CEOs of the insurance giants, Blue Cross, Health Partners, Medica, Health Partners, and UCare made $3,100,000, $2,400,000, $2,100,000, $929,900, respectively in 2017 (Kennedy, 2017). And these are just their base salaries, when stock options and other perks are factored in, you can take the base salary, double it (and then some), and then add a zero to the end. For example, in 2017, UnitedHealth Group’s executive chair made a base salary of $1,206,538, but with stocks and perks, total compensation was $26,975,932 (Kennedy, 2018).
b) How the “Ingenious” Formula Impacts Consumers’ Care
If low ROI was the upshot of Americans purchasing and utilizing health insurance plans to cover healthcare expenses, that would be disheartening, in and of itself. Unfortunately, low ROI is not the upshot; the upshot of Americans purchasing and utilizing health insurance plans is that deregulation of healthcare and the insurance industry have turned healthcare into a business, not a service, and the medical care consumers receive is suboptimal as a result (Frakt, 2018). Let me summarize: When people purchase insurance, 1) they lose money and 2) their healthcare is suboptimal. I don’t know about other consumers, but for me, there are only certain areas I’ll accept suboptimal (e.g., vehicle, internet carrier) and other areas I certainly won’t (e.g., healthcare, oxygen quality).
B. The New Era of Healthcare: Assembly Line Care
The changes that resulted from the deregulation of healthcare in the 1980’s turned healthcare into a business, a factory, if you will, and turned talented medical doctors into assembly line workers (Powers, 2017). Mental health providers are on the same trajectory. Remember, the deregulation led to a change in the insurance reimbursement metric such that services are reimbursed at a fixed rate, determined by the insurance company rather than the actual cost of services, and this led to a conflict of interest for providers and health care systems: Provide care according to best practices and potentially lose money, or cut costs and provide care as best you can within those cost constraints. At a basic level, this involves maximizing billable time and minimizing overhead, including unbillable time, medical services with low profit margins, additional staff, etc. Even prior to deregulation, the health insurance industry was motivated to maximize profit margins. The problem that was created with deregulation was that now both the insurance company and the provider/health care system were motivated to decrease costs and maximize profit margins, and the pressure placed on the provider/health care system by the insurance company to cut their costs, led to a conflict of interest, which resulted in a decrease in the quality of medical care provided. Indeed the U.S. is now ranked #1 in healthcare expenditure (Organisation for Economic Co-operation and Development, 2015) but #37 in healthcare system performance (Tandon, Murray, Lauer, & Evans, 2000).
1. Assembly Line Care in the Field of Physical Medicine
a) Assessment and Diagnosis
The employees of the insurance companies, the doctors and health care systems, are expected to conduct an efficient diagnostic assessment and provide an economically efficient treatment option, usually in under 15 minutes. After that, the provider is expected to complete another diagnostic assessment and provide a treatment option in under 15 minutes, and another diagnostic assessment and treatment option after that, and another diagnostic assessment and treatment option after that, ad nauseam. Not only does this place a tremendous amount of pressure on doctors, it’s not very effective. Not effective but very efficient, and that is the point. I know that an accurate diagnostic assessment for mental health is not possible within 15 minutes; the intake assessment takes around 2-3 hours and assessment is an ongoing process, throughout the course of treatment. Physical medicine is no less complicated, but yet the diagnostic and treatment processes have been severely abbreviated as a result of the insurance companies’ reimbursement policies.
b) The Western Medical Model and Health Insurance: Impact on Policies, and Ultimately, Patient Care
Not only are assessment and treatment abbreviated in physical medicine, other treatment practices are dictated by insurance company policy, not best practices. Western Medicine is designed to diagnose and treat problems at the pathogenic level, which means that the problem needs to progress to the expressed disease state before it can be identified and treated. Unfortunately, the issue is that the problem has already done a great deal of damage to the body at this point, and the damage is not always reversible nor is the problem always treatable at this point. The point at which a patient benefits most from a treatment intervention is earlier on, when the symptoms are more diffuse. Further, Western Medicine is designed to treat symptoms of disorder, not necessarily the underlying problem, so even after the problem’s symptoms have manifested, the actual problem often goes untreated. Quite obviously, the patient benefits most from the treatment of the underlying problem, not the symptoms, but this isn’t how the Western Medical System is set up. (And, nothing against the Western Medical System, it certainly has excellent merits; these are just the drawbacks.) There are schools of medicine (e.g., Ayurveda) and health interventions (e.g., nutrition and health coaching), designed to treat underlying problems, prior to pathogenesis, but the insurance industry will not cover these treatments. For example, Type II diabetes can be treated much more effectively early on, and even prevented by coaching interventions addressing diet and exercise. The problem is that our system is set up to wait until the actual disease has manifested before treatment, including diet, exercise and synthetic insulin administration, begins. At that point, insurance will reimburse diagnostic and treatment costs. Prior to that point, insurance will not cover effective treatments like health coaching or Ayurveda medical interventions. The insurance reimbursement system is set up to favor the Western Medical Model of diagnosis and treatment of the problem’s symptoms (not actual problem) when the problem reaches the pathogenic level.
Further, even after the problem becomes pathogenic and insurance is willing to cover treatment, the treatments are controlled by what the insurance company is willing to cover, and are complicated by the economic motivations of drug dispensaries (i.e., pharmacies). For example, Trintellix (i.e., vortioxetine) is a drug that works for both depression and anxiety, which are commonly comorbid conditions, and it is superior to a similar drug in its class, Effexor (i.e., venlafaxine), because it does not have the sleep side effects that Effexor does. And, as we know, those who suffer from depression and anxiety often experience sleep problems, so prescribing a drug that compounds their sleep problems is contraindicated. Unfortunately, the insurance companies require patients to have failed on the generic of Effexor, venlafaxine, which is cheaper, prior to authorizing payment for Trintellix. Alternatively, in order to avoid the sleep problem and follow the insurance company’s requirements, the prescriber could prescribe three medications, one for depression, one for anxiety, and one for sleep, rather than prescribing one drug, Trintellix. The prescriber is not allowed to practice according to best practices and the client does not receive the best treatment because of the reimbursement rules dictated by the insurance companies. This is the type of care consumers receive when they purchase a healthcare service from a third-party payer.
c) The Business of Healthcare and Your Pharmacist
Further thwarting patients’ receipt of superior drug treatments are the pharmacies. The pharmacies and pharmacists are incentivized to sell generic medications. When a consumer’s pharmacist informs them that there is a generic of the medication they’ve been prescribed, it seems like they are doing the consumer a favor, saving them money. In fact, they are saving the consumer money, but the consumer might not be getting the same drug they were prescribed, rather a similar medication from the same drug class, which may or may not be as effective as the drug they were prescribed. And, the part the consumer does not often realize is that the pharmacy’s profit margin is much greater for generics than for brand name drugs, so pharmacies are motivated to sell generic medications over name brands. Just as the generic is cheaper for patients to buy, it is also cheaper for pharmacies to buy, and they have more room to mark the drug up for profit than they do with brand name drugs, which are already quite expensive. This is why pharmacists push the sale of generics. One of my sources informed me that pharmacists don’t just push the sale of generics, they will actually tell patients that their insurance company won’t cover their brand name drug, so they need to go with the generic. Or, they’ll tell patients that they can’t get the drug in stock or that it will take several weeks to get the drug in their formulary, which isn’t true. The truth is that the patient needs a prior authorization in order to get the brand name drug, but the pharmacy withholds that information and tells them that the drug isn’t covered or that they can’t get it in their formulary (Brekke, Holmas, & Straume, 2010; J. Edwards, 2011).
2. Assembly Line Care in the Field of Mental Health
a) Assessment and Diagnosis
In mental health, the diagnostic assessment process typically takes 2-3 hours and continues throughout treatment; insurance only allows reimbursement for one, 53-minute session of diagnostic assessment, so any diagnostic assessment conducted after the initial session must be billed at the lower rate designated for therapy sessions. Providers are either forced to cram a 2-3-hour assessment process into 53 minutes or take a financial loss and provide a complete diagnostic assessment service at a lower rate. Arguable, a provider is not going to be as effective in providing an accurate diagnosis and formulating a treatment plan within a period of time that does not follow best practices. And, it is unfair to expect a provider to conduct an assessment over the time period proscribed by best practices with the trade off of accepting a lower pay rate. Further, how does this impact the provider’s feelings toward the client and the therapeutic alliance? Does the therapist feel some twinges of resentment about being undervalued by both the insurance company and the client?
b) The Western Medical Model: How it Influences Insurance Policies and Ultimately, Patient Care
As with physical medicine, in mental health, not only is assessment abbreviated, other treatment practices are dictated by insurance company policy, not best practices. Psychology also uses the Western Medical Model to diagnose and treat mental health concerns at the pathogenic level, which is necessary to receive reimbursement from insurance. Under this model, mental health disorder is made up of a constellation of expressed symptoms. Practically speaking, this means that providers must pathologize a survivor’s experience of abuse, neglect or other trauma by labeling the individual as “disordered” (Hari, 2018). And as with Western physical medicine, many mental health interventions are designed to treat symptoms of disorder, not necessarily the underlying problem, so the actual problem often goes untreated. For example, with a specific phobia, like arachnophobia, the presenting problem is a fear of spiders. The Western approach would be to utilize a cognitive behavioral protocol designed to address the fear of spiders and the other symptoms that go along with that (e.g., panic attacks, avoidance). However, as with physical conditions, the presenting problem is not usually the underlying problem. A fear of spiders is what we call a “safe fear”; it’s a controllable, concrete, external manifestation of a deeper problem, usually abuse, neglect or another trauma. The deeper problem is too terrifying to address, so the mind finds elaborate ways to manage the fear by displacing it on an object or creature such as a spider. Psychotherapy can certainly address the underlying problem, but the insurance system views these issues according to the Western Medical Model (disease-state model), and diagnosis, treatment and reimbursement have been tailored accordingly. Practically speaking, this means that a provider must diagnose and treat a “mental health disorder”, even if it is clear the person’s symptoms result from abuse, neglect, or other trauma (the actual problem), otherwise the insurance system will not cover treatment.
Frequency and duration of therapy, length of sessions, type of treatment, and not just diagnosis of problem as disordered, but allowable disorder diagnoses for treatment length are all dictated by what the insurance company will cover. Some insurance plans allow for more than one session per week and some allow only one. And, even if a client buys coverage with unlimited mental health sessions, allowing for increased therapy frequency and duration, there are loopholes that prevent this coverage from being truly unlimited; for example, requiring regular, written reports from the provider about client “progress” to determine if treatment continues to be “medically necessary”. Treatment of underlying problems like trauma, rather than treatment of expressed “disorder” symptoms, require more time and deep, complex interventions that do not fit with the brief, disease-state treatment models insurance companies proclaim are sufficient.
Some insurance companies will not reimburse for the standard, 53-minute therapy hour, and will only allow 38-minute sessions. For other companies, a 53-minute session is covered if a client has a certain diagnosis. This means that in order for a client to get the standard therapy hour, their provider needs to diagnose them with a condition that the insurance company has decided is severe enough to warrant a standard therapy hour. If they do not meet criteria for such a diagnosis, they cannot receive a standard hour of therapy. In some cases, the insurance contract has clauses potentially allowing longer treatment durations or session lengths, if the provider wants to complete a prior authorization. But, this is extra, unpaid work that’s placed on the provider and there is no guarantee that the prior authorization will be approved.
In response to health insurance’s “managed care” restraints on treatment, researchers began to develop briefer, symptom-focused treatment protocols to provide clients with some level of relief. Although these protocols have their merits and are helpful to alleviate distress in clients, they are not sufficient for many conditions and do not always address the underlying problem. This is by no fault of the treatment protocol; the treatment protocols are not designed to address the underlying problem, they are designed to address the symptomatology of an expressed disease state, just like most Western medical interventions. Curiously, even when providers utilize these protocols, developed to address insurance’s managed care constraints on mental health treatment, the insurance companies place further constraints on care. These “gold-standard treatment protocols” that researchers have developed and tested in clinical trial research, assume a standard 53-minute session, and as I discussed, not all insurance companies allow standard sessions. And some protocols, like Prolonged Exposure Therapy for Posttraumatic Stress Disorder (PTSD), which actually is designed to address the underlying problem (i.e., a traumatic event), rather than symptom presentation, require 90-minute sessions, which are not covered by insurance. The sessions lengths allowed by the insurance companies, fall short of what’s required by the “gold-standard treatment protocols”, developed through rigorous clinical trials, and providers are not able to provide clients with the best care available.
Furthermore, a source revealed to me that insurance companies believe that therapists are taking too long with clients and should be billing the minimum time necessary for procedures, like physicians do. More specifically, they believe that therapists should never need to see clients for a full, 53-minute session, and should only rarely see clients for ¾-length sessions (i.e., 38-52 minutes). Furthermore, the full to ¾-length sessions are viewed by the insurance companies as “extended” sessions and should only be necessary for the first few sessions. After that, sessions should never be longer than 16-37 minutes; following more of a maintenance model, and adhering to the minimum-time-necessary billing standard that physicians use. In my experience, the less than 15-minute consultation session I get with a medical doctor is not enough time to gather enough information for an accurate diagnosis and get my questions answered. For mental healthcare, designed to be a deep, introspective process, requiring high levels of self-disclosure and trust, a 16-minute session is an abomination. Not to mention the fact that it is around ¼ of the standard therapy session, 44 minutes shy of what is recommended by treatment protocols. So, even after attempts to adapt to insurance’s managed care constraints by developing and utilizing brief, symptom-targeting protocols, providers are literally not able to provide individual clients with the best level of individualized care; insurance companies control the type, amount, and frequency of treatment consumers are given.
C. A Rigged System
As mentioned earlier, the goal of health insurance is to take in more in premiums from consumers than they pay out in claims; in other words, the goal is to minimize their “medical loss ratio”. This is how they make a profit. It’s not fair to fault a business for trying to making a profit, but what also isn’t fair is that many people are under the impression that the health insurance system is fair and is designed to help them. This is a fallacy. Your insurance company cannot make money and ensure that you get your “money’s worth” out of your health insurance policy; these are diametrical goals. Consumers need to understand this. And providers need to understand this too because the implication for providers is that their employer’s goal is to pay them as little as possible. Indeed, in a Kentucky Supreme Court Case, Judge Osborne said, "Ambiguity and incomprehensibility seem to be the favorite tools of the insurance trade in drafting policies. It seems that insurers generally are attempting to convince the customer when selling the policy that everything is covered and convince the court when a claim is made that nothing is covered. The miracle of it all is that the English language can be subjected to such abuse and still remain an instrument of communication" (Osborne, 1970). Further, insurance companies utilize software programs nicknamed “denial engines” to go through claims to find clerical errors so they can increase the rate of legitimately rejected claims (McKennon Law Group PC, 2017). What’s more, a source informed me that the highest rates of claims denials were for mental health services and cancer treatment. I don’t want to jump to any conclusions about why these particular types of claims might have the highest denial rates, but I certainly have some ideas about this, and those of you reading this probably do too. Perhaps high expense to treat (high medical loss ratio) and limited ability of these populations to fight the claims denials might have something to do with this? I believe John Grisham wrote a “fictional” novel addressing these hypotheses.
This source’s information is not an aberration. In 2014, CBS’s 60-Minutes aired an exposé on mental health claim denials by health insurance companies. They found that the 11 doctors contracted by Anthem to review mental health claims had a denial rate averaging 90%; this denial rate persisted even when treating providers pleaded with the insurance claim reviewers to authorize additional care because of medical necessity. Following premature termination by the insurance company of provider-recommended mental health care, some of these patients died from causes linked to their conditions (Pelley, 2014). Disconcertingly, denials of such high-risk patients are common. Almost a quarter of all patients with chronic or persistent illnesses experience claims denials; and of these individuals, when their illness rose to the category of “serious”, the denial rate rose to 70%. What’s more, the rate of claim appeal is very low; data is scant but one piece of evidence suggests that 0.5% of denied claims are appealed. However, the reversal rate of denials is high, 40% on average (Government Accountability Office, 2011), leading some, such as McKennon Law Group PC, to state: “ This means health insurers routinely make the wrong decision and hope that their insureds do not pursue these claim denials…” (McKennon Law Group PC, 2017). Consumers are purchasing a third-party service to cover their medical expenses and those consumers who need it most aren’t allowed to reap the benefits of a service they paid for in good faith. How are mental health and medical providers supposed to provide treatment when the system is rigged? And, knowing this, why do we want to participate in a system where we and our clients are set up to lose?
II. Sustainability of the Current Third-Party Payer System: Financial and Inter/Intrapersonal Concerns
A. If Healthcare is More Expensive with Insurance, Why Do Consumers Buy Insurance?
1. The Power of Fear
Not only does health insurance offer a poor ROI and discourages best medical practices, I would argue that it actually makes healthcare more expensive. Healthcare is generally more expensive because the healthcare system is set up to be supported by the health insurance industry. When health insurance supports the healthcare system, consumers must pay the overhead of three entities, their doctor, their insurance company, and the billing person their doctor pays to navigate the convoluted claims process in order to receive payment from a third party. Business economics 101 would tell most of us that the best way to cut costs would be to cut out the middle man (health insurance industry). So, why do consumers buy their product if, logically, it’s such a terrible investment and it increases the costs of healthcare? Why do humans do lots of irrational things? Fear. Fear, and the invisible power of the status quo. Everyone is afraid that they will have a $100,000 or $1,000,000 health problem, they won’t be able to afford treatment, will die or bankrupt their family. That fear is valid. No one wants to die because they cannot afford medical treatment and no one wants to bankrupt their family. The problem is, in those instances in which consumers need a $100,000 or $1,000,000 medical treatment, there is still no guarantee that it will be covered by insurance. In fact, as discussed above, those with “serious” illness had very high claim denial rates, and many delayed or even forwent treatment because insurance denied their claims (Schoen, 2017). Further, many insurance plans have caps on medical expenses, usually around $1,000,000, so if and when consumers reach this amount, they lose coverage. If, rather than purchasing health insurance, consumers budgeted for health expenses each year and put that money into a savings account or a conservative mutual fund, they would end up with enough to cover that unexpected and highly unlikely medical expense (e.g., if consumers put $4000 into a mutual fund with a 10% growth rate, from ages 25-65, they would have almost 2 million dollars at age 65), rather than literally throwing that money away each year on an insurance plan that is set up to take in more than it pays out.
2. The Power of the Status Quo
The power of the status quo also explains why consumers continue to engage in the irrational behavior of buying healthcare at a financial loss via insurance. Consumers overlook the status quo because it is omnipresent and entrenched, essentially rendering it invisible. In order to make the invisible, visible, it needs to occur to consumers that there is something important to see and there needs to be a reason to look. Hopefully, this article has already established that there is something to see. So now the question is, “Why?” Why do consumers buy health insurance? Because it is financially beneficial? Because it allows consumers the best level of medical care? The previous arguments have established that neither of those conditions are true. So, why do consumers purchase and carry health insurance? Consumers carry health insurance because they are afraid, and also because that is what is done, what everyone does, and what everyone is supposed to do in order to receive healthcare (i.e., the status quo). Just because carrying health insurance is what is done, what everyone does, and what you are supposed to do doesn’t mean that it must be so or that it is a good idea. I think it is pretty clear that purchasing health insurance is not financially beneficial, but people’s fears and the momentum of the status quo are strong. Most consumers don’t seek to question how or why things are done, and if they do, they are often met with disapproval, “Why would you do that? That’s not what people do!” Such is the nature of challenging the status quo. Even if the status quo is successfully challenged, the next step is figuring out what to do instead, how to fill the vacuum left by the status quo. This is where many get stuck, if they’ve made it this far, and then begin retreating back to the status quo: “How am I going to go to the doctor if I don’t have health insurance? This is how things are done. I don’t know what to do instead.” The answer seems so simple, yet it is striking how many consumers cannot fathom an answer to this question: Pay for medical expenses directly with the money you would use to purchase an insurance plan and start a savings/investment account to cover future medical expenses. Consumers will save a small fortune using this approach. In fact, some doctors actually offer a discount to people paying with cash because they don’t have to pay a billing person to process the claim, cover insurance claim losses for other patients, cover the overhead of the insurance company, or cover the overhead of a large hospital (H. S. Edwards, 2017)
B. Health Insurance Facilitates the Undervaluing and Unsustainability of Mental Healthcare
Now, I discussed the fact that healthcare is generally more expensive because of the insurance industry. There is one segment of healthcare that is disproportionally inexpensive: mental healthcare. To those who are not mental health providers, this might come as welcome news, especially given the mental health crisis we have in this country—“Yay! Mental healthcare is affordable! Problem solved!” I would argue that the undervalued nature of mental healthcare actually contributes to the crisis. Our current, insurance-driven Western Medical Model of mental healthcare 1) is undervalued and financially unsustainable, and, 2) as discussed earlier, has turned mental healthcare into a business not healthcare.
Mental healthcare is undervalued and according to basic social psychology, we have a cognitive bias that says expensive = good/valuable and inexpensive = bad/not valuable (Cialdini, 2009); according to this bias, low reimbursement rates would lead people to believe that mental healthcare is not a valuable service. This conveys the message that mental health is not as valuable as physical health or even most people’s monthly car payment. The system is financially unsustainable because providers are paid poorly for the work they do, the annual salary per years of education is astonishingly low, there is a large discrepancy in pay for identical services between medical providers and therapists, the overhead is high compared to reimbursement, costs of training are high, many of the hours of required work are not reimbursed, there is no guarantee of payment or timely payment, and insurance contracts are limited.
1. Mental Health Providers are Paid Poorly Compared to Other Professionals
a) M.D. versus Ph.D. Salary
Table 1 (below) highlights salaries across several professions. These are salaried positions, so they are not directly tied to insurance reimbursements, but I include these to illustrate the incredibly low pay rate for mental health professionals compared to other professionals. Later, I will discuss the insurance reimbursement rates for mental health, factoring in overhead; these rates are much lower than the median salary listed for a Ph.D.-level psychologist, and ultimately, are lower than the pay rates for every other profession listed in Table 1.
Let’s take a look at what certain professionals are paid and let’s consider whether mental health providers’ wages are fair. According to PayScale.com, doctoral-level psychologists make an average of $74,000 per year and masters-level therapists make an average of $43,000 per year. By comparison, psychiatrists, make an average of $195,000 per year. Physicians in the lowest paid medical specialty, family medicine, make an average of $175,000 per year (PayScale). The table also highlights required years of education to practice in each field (Rubin, 2010). As illustrated, doctoral-level psychologists are required to complete one year less training than a family physician and make only 2/5 of the salary that a family physician makes (Study.com). That is a major discrepancy for only one year of training.
b) M.D. versus Ph.D.: Discrepancy in Reimbursement for the Same Service
Further highlighting the discrepancy in pay between physical medicine and mental health is a direct comparison of reimbursement rates between M.D.s and mental health providers for the same mental health service. When billing for the same service, physicians are reimbursed 50% more by the insurance companies than therapists (Gold, 2017). This is very surprising given the fact that the same service is performed. And it is especially surprising and dare I say, disconcerting, that the individual with the highest level of training in a given service area (the therapist) is paid 50% less than the individual with virtually no training in a given service area (the physician). If we look at the inverse, therapists providing medical services, such as medication management, in which therapists have very little training, just as a medical doctor has very little training in providing therapy, therapists are prohibited from performing the service at all, and will most definitely not receive reimbursement for providing the service.
c) Therapist versus Life Coach: Discrepancy in Salary for Similar Services
I didn’t include life coaches’ salaries in the table below, but I think it’s important to note the discrepancy in salary here, given that they provide similar services. By definition, “life coaching is the process of helping people identify and achieve personal goals. Although life coaches may have studied counseling psychology or related subjects, a life coach does not act as a therapist, counselor, or health care provider, and psychological intervention lies outside the scope of life coaching” (Wikipedia). In other words, therapists provide the same service as coaches and much more; therapists have received required, specialized training in human behavior and therapeutic interventions. If logic drove the world, I would conclude that therapists must receive a much higher salary than coaches, given their level of training, the liability involved with their jobs, and the breadth and depth of the services they are able to provide. As it is, logic does not drive the world. In a brief search of coaching services in the Twin Cities metro area, I found that coaches may or may not have advanced degrees, offered similar services to therapists (with the exception that therapists provide a breadth and depth of service that coaches are unable to provide), and charged between $200-667 per session hour for their services (Burza; Marver; Stimpson). By comparison, as I will discuss below, most insurance companies will reimburse no more than $130 per hour for a Ph.D.-level therapist. Therapy rates ranging from $200-667 per session hour are virtually nonexistent, even in the private-pay sector.
Initially, this discovery made me feel very resentful toward life coaches, the insurance companies, and society for undervaluing our profession. After tracking down the source of my resentment and seeking to understand it, I realized that there’s no need to use my energy on resentment, rather, there’s some very valuable information in this discrepancy (McLain, 2018). Specifically, people do value the services therapist provide and are willing to pay a healthy, out-of-pocket rate for them. The mental health field can learn from life coaches about how to market services and advocate for better rates of pay.
d) Discrepancies in Salary Between Mental Health and Other Professionals
Individuals in other professions with equivalent or fewer years required training than that required for doctoral-level or masters-level mental health professionals make substantially higher salaries, such medical doctors (as discussed above), attorneys, and investment bankers. If we look at only masters-level therapists, every profession listed, with the exception of a dog trainer, makes a higher or equivalent salary, and even a dog trainer doesn’t make much less than a therapist. And, when we look at insurance-based salaries, every profession listed makes more than a masters- and doctoral-level therapist. To better compare education level by salary, I’ve included a figure for annual salary per years of education. It is commonly thought that higher education increases overall salary, and appears to be financially advantageous over time, but in the one-year snapshots highlighted in this table, annual salary per years of education does not appear to be a good investment of time or money. This is most notable for graduate degrees in mental health, and especially for masters-level therapists, who make similar or lower salaries than those with similar or fewer years of higher education, such as attorneys, investment bankers, insurance brokers, commercial truck drivers, machinists, and psychics (How to Become; PayScale; Study.com).
Let me highlight one discrepancy in particular: The person who sells consumers their insurance policy makes more than their masters-level therapist and makes only 14,000 less than their doctoral-level therapist, despite their therapist’s 7-10 additional years of training (Study.com); and if we consider salaries of therapists credentialed with insurance (discussed later), the insurance broker makes much more than both masters-level and doctoral-level therapists. Does anyone see something wrong with that? Consumers are paying the person they buy their insurance policy from more than they are paying their actual provider. It certainly speaks to where the bulk of the consumer’s investment in their insurance plan goes (i.e., to the costs of administering the plan, not in paying for actual medical services). In my opinion, the truth of these discrepancies is insulting, marginalizing, and sad for the field of mental health. I think these discrepancies reflect the values of our society. We place more value on manufacturing a widget, how fast our money can grow, moving our consumer goods across the country, and almost as much value on the training of our pets than we do on our well-being. I suppose this is evident from the tenor of our country’s spirit, but despite our despondency, we have failed to fully see and address this discrepancy. Logically speaking, how happy is a society going to be who places consumerism over well-being?

2. Mental Health Provider Salary Under the Insurance Reimbursement Model
Not only are the salary discrepancies between mental health professions and other professions disconcerting, the numbers I’ve discussed aren’t the full picture. The mental health salaries I’ve listed above are median salaries and are not the actual salaries for a therapist in private practice, accepting insurance. So, the numbers above include therapists who work for agencies, the VA system, for corporations, universities, et cetera; the pay rates among these sectors varies significantly.
a) Substantial Salary Reductions Over Time
One thing you might like to know before I discuss current insurance reimbursement rates, is that reimbursement rates for therapists used to be much higher than $130 per session (which is at the higher end of the reimbursement spectrum), even without adjusting for inflation. Twenty-four years ago, Ph.D.-level therapists received insurance reimbursements that were higher than the current, $130/session, receiving reimbursements from that same insurer of $150/session, which is the equivalent of $253/session in 2018 dollars ("U.S. Inflation Calculator,"). With deregulation of healthcare and the transition to managed care, managing the costs of physical and mental healthcare, the reimbursement rates have dropped substantially. So, how can insurance companies get by with reducing reimbursement rates by 51% without anyone noticing or complaining? A combination of factors such as not adjusting for inflation, making small rate decreases over time, and the naïveté of new generations of therapists, unfamiliar with the old ways (and reimbursement rates), have made the reductions nearly invisible; furthermore, mental health providers do not have any representation to advocate for fair wages, such as physicians do with the American Medical Association (Powers, 2018). Another factor, that could take up an entire article, is that the field of psychology has transitioned from being a male-dominated field to a female-dominated field, which is not the case for physical medicine; physical medicine continues to be male dominated (Kaiser Family Foundation, 2018). In 1970, around 30% of all Ph.D.’s in psychology were awarded to women; in 2008, over 70% were awarded to women (Willyard, 2011). And, from 2005 to 2013, the number of active female psychologists in the workforce rose 10%, from 58% to 68% (APA Center for Workforce Studies, 2015), which is a fairly rapid shift. The gender disparity in salary in this country is undeniable (Miller, 2016). The shift to a female majority in the field of psychology over time may help explain the shift (decrease) in reimbursement rates over time.
b) The Financial Realities of Reimbursement Rates
(1) Realistic Client Contact Hours per Week, Vacation Time, and Overhead
When we first glance at reimbursement rates for insurance credentialed providers, the rates might not seem too bad: Insurance companies A, B and C pay $130 per 53-minute session whereas insurance companies D, E and F pay $94 per 53-minute session for a doctoral-level psychologist. So, at first glance, it would appear that mental health providers are making $94-$130 per hour and at 40 hours per week, that’s a pretty great salary: $195,000 to $270,000 per year. Unfortunately, those numbers do not reflect reality. Therapists cannot provide 40 hours of therapy per week, provide a high level of care, and have time to take care of themselves. Therapists also cannot work 52 weeks per year, provide a high level of care, and take care of themselves. Further, the $195,000 to $270,000 annual salary does not include overhead.
The annual salary of an insurance credentialed provider looks much different if we take a more realistic view of the number of clients a therapist can see each week, the number of weeks of vacation a therapist takes each year, and the overhead involved with running a small medical practice, which is a complex figure to accurately compute. Depending on the type of therapy a therapist does, the types of clients a therapist sees, the therapist’s level of experience, the amount of internal process work a therapist has done, a therapist’s sensitivity and attunement level, and how much a therapist believes in role modeling boundaries and self-care in their business, most therapists see between 10-20 clients per week; some see as many as 25, but that is usually the upper limit. And, I suspect that many therapists may want to see fewer clients than they actually see but feel that they need to see more clients because of financial constraints, social comparison, and some beliefs about martyrdom.
In addition to number of clients seen each week, vacation time must be subtracted from the equation. The American standard for vacation time is two weeks per year. I don’t think that two weeks is healthy for any American and would argue that therapists need to take substantially more vacation time than the average American if they want to prevent burnout and provide a high level of care to their clients. I believe that therapists should take a minimum of six weeks of vacation time each year and preferably even more than that; Casey Truffo recommends eight weeks (Truffo, 2007). (I personally take 12 weeks each year and have noticed a reduction in burnout and increase in my ability to provide quality care.)
After computing number of clients seen each week and weeks of vacation per year, we need to compute basic overhead. My basic overhead, per therapy hour, per week is around $40; I’ve heard other therapists quote a similar number, but I would encourage the therapists reading this to calculate their individual overhead figure. Basic overhead includes costs such as rent, transportation, office supplies, therapy materials, phone, website, advertising, billing, malpractice insurance, licensing, continuing education, personal therapy, consultation (e.g., business, client, legal), networking, etc. As I mentioned, overhead is a complex number. I’ll first discuss estimated salary with basic overhead, then I’ll discuss aspects of overhead that are often overlooked.
(2) Wide Variability in Salary, Independent of Therapist Efficacy and Effort Level
We’ll look at two therapists, both with doctoral degrees, in different scenarios in order to get a better picture of the salary range. Therapist B is credentialed only with insurance company F, makes $94 per session, sees 10 clients per week, works 46 weeks per year, and pays $40 in overhead per session, per week. Therapist B’s actual reimbursement rate per session is $94-40 = $54 per session. At a rate of 10 clients per week and 46 weeks per year, Therapist B’s annual salary is $24,840 per year. Therapist A was able to get a contract with one of the best health insurance companies in the state, so Therapist A receives $130 per session. Therapist A sees more clients per week, 20, and works 46 weeks per year, and pays $40 in overhead per session, per week. Therapist A’s actual reimbursement rate per session is $130-$40 = $90 per session. At a rate of 20 clients per week and 46 weeks per year, Therapist A’s annual salary is $82,000 per year. That’s not too bad.
Pay rates vary widely, and somewhat arbitrarily, depending on whether insurance companies with higher reimbursement rates and higher enrollment numbers are offering contracts in a particular area; this variability is not tied to treatment complexity, therapist effort level, or therapist efficacy. Let’s consider treatment complexity, which is tied to effort level, using the hypothetical therapists from above. Therapist A lives in an area where Insurance Company A is offering new contracts at a $130 rate; Therapist A’s treatment specialty is personal growth; she utilizes a surface-level, goals-based treatment process, and her clients tend to be very high functioning individuals, diagnosed with Adjustment Disorder, Unspecified. She is able to see 20 clients per week. Therapist B lives in an area where only Insurance Company F was offering new contracts at a $94 rate. Therapist B’s treatment specialty is trauma treatment; she utilizes a deep, internal processing approach with clients that is effective but intense and emotionally draining for her and her clients. Her clients are typically diagnosed with Posttraumatic Stress Disorder (PTSD) and Major Depressive Disorder (MDD). Because of the intense work she does with a high-risk population, Therapist B is only able to see 10 clients per week, while still ensuring a high level of client care and time for personal care. Both therapists are great at what they do, but for reasons completely unrelated to their efficacy, treatment complexity, and effort level, Therapist A makes much more than Therapist B. In fact, Therapist B can’t even pay her bills.
(3) Often Overlooked Aspects of Overhead
(a) Healthcare
Now for the aspects of overhead that are often overlooked: healthcare, retirement, self-employment tax, and student loan debt. Despite the fact that Therapists A and B technically work for the health insurance companies, because they are contract employees, they don’t receive any of the benefits that go along with the drawbacks of employment by a large company, like health insurance or retirement. So, both therapists have to buy their individual health insurance on the open market. If we assume that both therapists are healthy, nonsmoking women in their mid-thirties, and are only buying individuals plans, they can expect costs ranging from $3277 to $4784 (only covering premium with no attempt to use the policy to pay for healthcare) to $9,877 to $12,134 (cost of premium plus attempts to use the policy to pay for healthcare via deductible) per year (Health Partners Insurance). After paying for health insurance, Therapist A (initial salary of $82,000) is bringing home between $78,723 and $69,866 (depending on whether she actually used the insurance coverage or not), with an average of $74,295; Therapist B (initial salary $24,840) is bringing home between $21,563 and $12,706, with an average of $17,135.
(b) Retirement
Typical retirement contributions by employers use a match system of 50 cents per employee dollar contribution up to 6% of employee’s salary (Brandon, 2010). The insurance companies’ contract employees are not eligible for an employer match, so we need to determine not only out-of-pocket retirement costs, but also the employer match amount as lost salary. If Therapist A makes $82,000 per year, and contributes 6% of her salary, that would be $4,920; the missing employer match is $2,460. In order to be on pace with her non-contract employed peers, Therapist A would need to budget a $4,920 personal contribution plus the $2,460 missing employer match; a total of $7,380. If Therapist B makes $24,840 per year, and contributes 6% of her salary, that would be $1,490; the missing employer match is $745. In order to be on pace with their non-contract employed peers, Therapist B would need to budget a $1,490 personal contribution plus the $745 missing employer match; a total of $2,235.
How much are Therapist A and Therapist B making after paying for their health insurance and retirement benefits out of pocket? If we take Therapists A and B’s average salaries after paying for insurance coverage, $74,295 and $17,135, respectively, and subtract retirement contributions, $7,380 and $2,235, respectively, we get a salary of $74,295-$7,380 = $66,915 for Therapist A and $17,135-$2,235 = $14,899 for Therapist B.
(c) Self-Employment Tax
In addition to regular income taxes, self-employed individuals have to pay self-employment tax. The self-employment tax rate is 15.3%, which covers Medicare and Social Security. For traditional, non-contract employees, the Social Security and Medicare tax rate is 6.2% for each individual and 6.2% for each employer (Internal Revenue Service; Internal Revenue Service). Again, despite the fact that Therapists A and B are technically employed by the health insurance companies, they are contract employees, so the insurance companies do not pay part of the tax; Therapists A and B have to pay the entire amount. After paying for insurance and making a retirement contribution, Therapist A has only $66,915 remaining annual salary and Therapist B has $14,899. Self-employment tax contributions for Therapist A and Therapist B are $10,238 and $2,280, respectively, leaving therapist A with a salary of $56,677 and Therapist B with a salary of $12,619. If the therapists had been actual employees of the insurance companies, they would have reduced their tax rate by 9.1%, which is a savings of $6,089 for Therapist A and $1,355 for Therapist B.
(d) Student Loan Debt
Another aspect of overhead that’s often overlooked in overhead calculations is student loan debt. Therapists A and B both have Ph.D.’s which means they paid for at least 10 years of formal education and training (including their postdoctoral residency). The amount of student loan debt depends on type of graduate program attended, scholarships, outside assistance, etc., but few individuals with graduate-level training can escape student loan debt. Just as any other small business would include conferences, continuing education, and trainings in their overhead, mental health private providers should include their most essential training cost, their degree, in their practice’s overhead. Right now, therapists in private practice have some options for loan repayment, including making full payments or applying for an income-based reduced payment. Making a full payment is exactly what it sounds like, after loans come out of deferment, individuals follow the payment amount and schedule the lending company prescribes. The second option, an income-based reduced payment, uses a formula based upon income to determine the payment amount an individual can afford. At the end of 25 years, the remaining amount of the loan is discharged as income, not forgiven (as many people believe). In other words, individuals utilizing the income-based repayment plan will need to pay taxes on the remainder of the loan amount, and if they were only able to make small payments because their income was not commensurate with the amount of training and student loan debt they acquired, that loan amount will have grown astronomically. Let’s apply the two scenarios, making regular payments and utilizing an income-based repayment plan, to our hypothetical therapists (See Table 2).
As I mentioned, both Therapists A and B have doctoral degrees, both received scholarships, but with personal expenses and school expenses over the course of earning their degrees, they ended up with $205,000 in student loan debt. (Note: If credit cards or personal loans were used to cover expenses during school and/or the lean times in a new private practice, please include that debt in overhead calculations; that is considered part of training/business expenses.) After Therapists A and B paid for health insurance, retirement and self-employment tax, Therapist A is left with $56,677 annually and Therapist B with $12,619 annually.
In Scenario 1, the therapists make payments according to the amount and schedule prescribed by the lending company, which is $2,245 per month, or $26,940 annually, until the loan is paid off (approximately 10 years). After making required payments, Therapist A is left with $29,737 annually and Therapist B is left with -$14,321 annually.
In Scenario 2, the therapists make income-based payments and at the end of 25 years, the balance is discharged as income. Therapist A’s income-based payment is $404 per month ($4,848 annually); after making this payment, Therapist A’s annual income is $51,829. At the end of 25 years, the remaining balance to be discharged is $304,307 and according to the tax calculator, Therapist A will pay $89,438 in taxes on that amount. How is Therapist A supposed to come up with $89,438 on a salary of $51,829?! If anyone is wondering which scenario is most fiscally advantageous, it’s Scenario 1, making the full payments each month. If Therapist A picks this option, Therapist A will pay a total of $273,890 on the original loan of $205,000; if therapist A picks Scenario 2, the income-based repayment plan, Therapist A will make $208,876 in payments plus will pay the income tax of $89,438 for a total payment of $298,314 on a $205,000 loan; that’s a savings of $24,424, utilizing Scenario 1. (If the total numbers seem off, it’s because the repayment plan considers income growth in the algorithm and I didn’t go into detail about that here.)
In Scenario 2 with Therapist B, her income-based payment is $0 per month because her income is so low; as such, her annual income remains at $12,619. At the end of 25 years, the remaining balance to be discharged is $512,500 and according to the tax calculator, Therapist B will pay $181,339 in taxes on that amount. Again, how is Therapist B supposed to cover a $181,339 tax bill on a salary of $12,619?! If anyone is wondering which option is most fiscally advantageous for Therapist B, it’s Scenario 2, taking the income-based repayment plan. If Therapist B picks this option, Therapist B will pay a total of $181,339 on the original loan of $205,000; if Therapist B picks Scenario 1, the payment plan prescribed by the lending company, Therapist B will make $273,890 in payments on the original loan of $205,000. Scenario 2 ($273,890) - Scenario 1 ($181,339) = $92,551 savings; further Scenario 2 offers a $23,661 savings on the original loan ($205,000-$181,339; (Kirkham, 2017; Smart Asset).
Table 1 provided a metric for comparing the value of higher education (i.e., salary per years of education) and highlighted the low monetary value of education in the field of mental health. What Table 1 didn’t highlight was the amount of debt that accumulates with each year of education. So, not only do mental health providers spend employable years of their life not working so they can receive training and are paid poorly when they graduate, mental health providers incur significant levels of debt during that time. The discussion above highlights the practical impact of this training debt. I hope that the discussion made it clear that someone with 10 years of education and a significant amount of student loan debt cannot afford to accept the reimbursement rates offered by the insurance companies. A salary ranging from -$14,321 to $51,829, at best, just covers basic life expenses and at worst, puts the “earner” into compounding debt each year. And, it is completely unacceptable for someone with 10 years of higher education. We all need to ask for more. We certainly deserve a better salary than -$14,321 to $51,829. I mean, seriously, there’s a negative number in this salary range! What are we doing to ourselves?

(e) Unbillable Hours
A final often overlooked aspect of overhead is unbillable hours. It’s important to note that the number of client hours billed per week does not reflect the actual number of hours worked per week. If therapists are credentialed with insurance, they can estimate that they will spend an additional 30 minutes per client, per week on various activities associated with insurance (e.g., credentialing, contracting, paperwork to authorize additional sessions, going through EOBs to make sure sessions were reimbursed, determining client portion of payment and collecting payment from clients, calling the insurance companies to discuss discrepancies, being upset about how much additional work they need to do to get paid, etc.). Therapists are probably spending at least another 30-60 minutes per client, per week, on unpaid activities associated with their practice (e.g., session preparation, notes, scheduling, marketing, networking, referrals, consultation, training, internal process work, etc.). Using these numbers, therapists who accept insurance spend 60-90 minutes, per client, per week, outside of session on client-related activities. Taken together, these therapists are spending between 2 and 2.5 total hours per client, per week on practice-related activities, or 20-50 hours per week total, depending upon if the therapist sees 10 or 20 clients per week. This time doesn’t include the self-care time essential for recharging to show up fully for work with clients. I will discuss that later.
To reiterate, providers who accept insurance spend 5-10 hours each week (depending on client load), above and beyond their regular duties, just dealing with the insurance process. That is time that is given away: your precious time, for free! Let’s look at what the reimbursement rates look like after paying basic overhead and after factoring in the unbillable time required to accept insurance. Insurance company A reimburses at $130 per billable hour and Insurance Company F reimburses at $94 per billable hour; each company requires .5 unbillable hours per billable hour, for a total of 1.5 hours of required work, billable and unbillable; overhead is $40 per billable hour. That means that the hourly rate for Insurance Company A is $130-$40=$90 divided by 1.5 total hours; that number is $60 per hour. The hourly rate for Insurance Company F is $94-$40=$54, divided by 1.5 total hours; that number is $36 per hour. The actual reimbursement rates are much lower than they appear in the contract you sign each year, and although Insurance Company A’s rate still doesn’t look that bad; Insurance Company F’s rate of $36 per hour is pretty low. And, wouldn’t it be nice if your contract reflected your actual hourly rate of reimbursement? I think that’s called full disclosure.
If we take this a step further and enter in the total time spent on insurance-, practice- and client-related activities per week, which is 2-2.5 hours per client, the numbers are much lower. The hourly rate under contract with Insurance Company A is $130-$40=$90 divided by 2.5-2 total hours, which is $36-$45 per hour. The hourly rate under contract with Insurance Company F is $94-$40=$54 divided by 2.5-2 total hours, which is $21.60-$27 per hour. Furthermore, I’ve chosen to present these numbers with only the basic overhead and haven’t included the other factors such as number of billable hours that are practical in a week, vacation time, or the often overlooked aspects of overhead such as benefits, self-employment tax, and student loan debt. So, make no mistake, therapists are not actually making the $21.60-$45 hourly rate I used for illustrative purposes here.
c) Additional Considerations
(1) No Guarantee of Payment or Timely Payment
Not only does accepting insurance require an additional 30 minutes per client per week, there is no guarantee that a provider will ever be paid by the insurance company, and most certainly, the provider will not be paid in a timely manner. For those of us familiar with the process, claims are typically processed and paid out within 1-4 months and sometimes are never paid, despite significant time and effort to receive reimbursement. I don’t know a single provider who has been paid for 100% of the legitimate claims they’ve filed. There are many reasons given by the insurance companies for these delays in payment and nonpayment of claims: the claim wasn’t received, the claim wasn’t received on time (even if it actually was submitted on time), there was some sort of error in processing the claim, there was a problem with their system, the diagnosis isn’t sufficient for that service, inaccurate coding by doctor, incomplete or inaccurate insurance information, lack of prior authorization or referral, the client’s specific insurance policy does not cover a 53-minutes session, it only covers a 38-minute session (after the provider has already provided a 53-minute session), the insurance company needs proof that the service is medically necessary, (McKennon Law Group PC, 2017), or my favorite, the claim was approved but the insurance company “forgot” to issue a payment. It would almost seem as if the system was set up to find ways to not pay claims (see section “A Rigged System” and its description of “denial engines”).
How many people would stay at a job where their boss didn’t pay for a full 1/3 of their working time (i.e., 60 minutes in session, 30 minutes out of session to bill)? How many people would stay at a job where requests to receive their paychecks are frequently denied? How many people would stay at a job where it could take 1-4 months to get a paycheck? Who would agree to learn and follow a complex billing rubric, with hundreds of variations, that can constantly change? Should someone with a doctoral or master’s degree put up with all of this for compensation between -$14,321 to $29,737 per year?
(2) Contracts are Limited and Consumers May Switch Carriers at a Moment’s Notice
Another caveat is that, in some metro areas, such as the Twin Cities and Duluth, Minnesota, some of the most popular insurance companies (i.e., those with high enrollment numbers) with the best rates are not offering any new contracts. Any therapists who decide to make the leap into private practice will not be able to get credentialed at the higher, $130 rate or will have to join a group practice in order to credential with those companies, which usually involves a much higher rate of overhead. There may be other insurance companies offering the higher, $130 rate, but they don’t have the same enrollment numbers, so it is more difficult to get new clients. Not to worry, Insurance Company F is almost always offering new contracts at their $94 rate, and has pretty decent enrollment, so therapists can see 20 clients per week and make between $21.60 and $27 per hour, before taxes, benefits, and student loan payments. Not bad for a Ph.D.
Finally, even if a therapist is able to get credentialed with an insurance company (or companies) with high enrollment and higher reimbursement rates, if their client switches insurance carriers, and the therapist is not credentialed with the new company, the therapist will lose that client (and that income). Or, if the therapist is credentialed with the client’s new insurance carrier, the therapist will have to accept that carrier’s rate, which could be much lower than the rate they were previously receiving. Further, if a client stays with the same carrier, but changes plans, the client may no longer be able to afford their co-pay/coinsurance/deductible and may terminate therapy, and the therapist will experience a loss of income.
C. Inter/Intrapersonal Concerns and Sustainability for Providers
1. The Consequences of Unhelpful Beliefs About Money and Martyrdom: Burnout and Devaluation of Mental Health
Unhelpful beliefs about money and helping people lead to burnout. Specifically, there’s a belief in society that people shouldn’t expect payment for good deeds, and if someone does, that is bad, and that person is also bad. Along these lines, there are beliefs that money is bad or represents greed (Truffo, 2007). Interestingly, we all need money to survive, so these beliefs create a double bind. An extension of these beliefs about money relates to therapists’ work as therapists: If therapists make their living providing good deeds to people, therapists are bad if they expect to be paid well, if at all (McLain, 2016). The problem is that this belief is not practical or even very useful. The belief actually contributes to a larger problem, martyrdom. Society loves martyrs; they are good; they died for their cause; we should all aspire to be them. The problem is, martyrdom is not sustainable, in fact, ask any martyr how martyrdom turned out for them and you’ll learn that it’s not sustainable. Putting others’ needs ahead of our own leads to all sorts of unhelpful dynamics that can be played out unconsciously, but the main issue I’m going to point out is that it leads to burnout.
Burnout is a process that starts with putting others’ needs ahead of our own, telling ourselves that we are okay with it, attempting to push down feelings of resentment, unsuccessfully pushing down/fighting off feelings of resentment, and ends with feeling embittered and exhausted. Facilitating martyrdom, resentment, embitterment, and exhaustion is the antithesis of the therapeutic process. Not only that, it’s poor role modeling for clients. In putting clients’ needs ahead of therapists’ needs, therapists create an unsustainable professional existence, not only for therapists as individuals but for the field. Credentialing with the insurance companies requires therapists to make sacrifices of their time and money, in order for others (clients) to utilize their insurance plans. Therapists are expected to work a portion of the week for free and accept a salary that is not sustainable or commensurate with their training level to benefit another person. If that isn’t martyrdom, I’m not sure what is.
Not only is the salary insufficient, it perpetuates the belief that therapy is not valuable. By accepting a rate of pay that is not sustainable or commensurate with their training level, not only are therapists martyring themselves, therapists are perpetuating the belief that therapy is not valuable. Therapy is invaluable. Therapists help heal people’s pain and change their lives. I think many therapists fail to recognize this. Most therapists feel called to this work, find that their work just comes naturally to them, and can’t imagine working in another profession, which may be why therapists don’t see the value in their work. Casey Truffo (2007) talks about this in her book, Be a Wealthy Therapist; she discusses the idea that helping people heal themselves is normal to therapists, just like drinking water, and therapists fail to see what the fuss is all about. Normalizing the value of therapeutic work is also likely why therapists don’t feel they need to be paid more, don’t see the costs involved in their work, and focus on what others need, not asking for what they need (or believing that they deserve to ask). When therapists credential with insurance companies, they don’t have the ability to ask for more, more money or more time to take care of themselves, because they are bound by the pay rates and time requirements of the insurance process.
2. Self-Care is a Necessity Not a Luxury
Therapists asking for more time and money to take care of themselves isn’t a luxury, it’s a necessity to create a sustainable individual existence and sustainable field. When therapists get home after a full day of clients, they often have nothing left to give and their work can have a detrimental impact on their personal lives. Remember Therapist B? I discussed that her specialty is in trauma and she utilizes a therapeutic orientation that requires deep, internal processing of trauma with clients; this work is exhausting and heartbreaking. Depending on her client load and the issues addressed, some days when she gets home, she can only sit on the couch and stare like a zombie. She’s not able have a conversation, make dinner, or engage with her partner or children in a meaningful way. On really tough days, she cries, is crabby, and needs a lot of emotional support from her partner; it might take her a day or two to get back to feeling like herself again. On really, really tough days, she experiences harassment, emotional abuse, boundary violations, and even feels scared for her life and safety. And she has reason to feel scared, one of her colleagues was killed by a former client. The risks she takes and the sacrifices she makes in the service of helping others are real.
It is impossible for this work not to affect therapists as individuals, no matter how great their boundaries are. This is because the therapeutic process works when therapists are able to fully engage with their clients and truly feel their experience alongside them; this process is emotionally draining. If you don’t work as a therapist, you can probably relate if you’ve ever supported a friend or family member through a painful time. The process takes an incredible amount of emotional energy and leaves you depleted. This is a huge sacrifice to make for another person. I’m not saying people should stop supporting loved ones or stop providing therapy, I’m saying that therapists need consider the value of their work and the costs they incur to their health and personal lives. And, if therapists want to continue to do their work effectively, they need to make sure they are taking care of ourselves in a way that recharges their depleted emotional energy. This also means being compensated in a way that prevents therapists from feeling resentful about the sacrifices they are making to help others, and that gives therapists the ability to take incredibly good care of themselves, in order to recharge their energy.
It might be helpful to conceptualize therapists’ work schedule and compensation rates like the work schedule and compensation rates of professional athletes. Like professional athletes, therapists’ visible work, the hours they are paid for (direct client contact hours) are a tiny proportion of the work they actually do in order to show up as therapists (Powers, 2017). Prior to starting in practice, therapists spend around a decade training to become therapists. After that, therapists spend hours each week, training to continue their work as therapists, not only doing formal consultation and training, but doing individual process work, so they can show up for their clients without letting their own issues cloud their perceptions and take up too much space in the therapy room. Therapists also spend hours each week taking time for self-care to recharge their emotional energy. Therapists need to be paid well for their time “on the field”, because the rest of their time spent working is not compensated.
The amount and type of self-care time therapists take needs to be commensurate with the amount and type of emotional output. In other words, self-care for a therapist needs to be on a different plane than self-care for the average person. By self-care “on a different plane”, I mean retreats, long, restorative weekends with best friends, trips to beautiful places, gourmet meals, massages, hours and hours spent in favorite activities without any other responsibilities, anything that is self-indulgent. These activities need not be material or expensive but they need to be restorative and about taking care of only the therapist, and not partners, kids, family members, or friends. Unfortunately, insurance reimbursement rates do not allow therapists to create a sustainable income and take the time necessary to take care of themselves. Therapists end up needing to stretch their boundaries to see as many clients as possible to earn a decent living, and doing so does not allow therapists to practice from grounded place of their needs being met and energy restored.
3. Diffusion of Responsibility
When people use an insurance plan to pay for medical or mental health services, three parties are involved in the care of one party and a diffusion of responsibility takes place. This diffusion of responsibility facilitates a fallacy that someone else is paying for the client’s services: “Insurance is covering it.” The client is ultimately paying for services via the insurance plan they’ve purchased, but the onus of responsibility rests on a third party, or appears to rest on a third party. Why does this matter? Well, when someone pays directly for a service, there is a clear, reciprocal exchange. I provide a service and you are responsible to pay me for the service. When a third party is involved, the responsibility is diluted or “diffused”. The client purchases a financial service from the insurance company, receives a healthcare service from a therapist, and the third-party financial service (insurance company) is required to pay the provider for the healthcare service that was provided to the client. Do you see how complicated that is? The client is no longer responsible to pay directly for the healthcare service they received; the financial service they hired is responsible to pay for that service.
Further complicating this exchange is the fact that the insurance contracts are incredibly complicated; most people do not understand the contracts (McKennon Law Group PC, 2017) or their financial responsibility. So, when the third-party financial service doesn’t cover part or all of the healthcare service for some reason, perhaps the deductible has not been met or they claim that the service isn’t covered under the umbrella of the financial service, who takes responsibility? Theoretically, the client does, but what happens in practice? The client often feels jilted by their insurance company because they are operating under the false belief that the insurance company is supposed to cover their healthcare expenses, and the client is upset (often with the provider) because now they have to pay the provider for a service they can’t afford, and likely wouldn’t have purchased if they’d known they’d have to pay for it directly. And, what happens when the insurance company says, “I am not going to pay for the healthcare service you received because your provider didn’t follow our convoluted rules,” (i.e., your provider provided your healthcare according to best practices, rather than according to most cost-efficient practices) and now you are responsible for full costs? The client is not going to believe that it’s their responsibility to pay for their healthcare services because their insurance company told them that their provider did something wrong. This damages both sides of the therapeutic relationship: The client feels that their provider has cheated them and the provider feels their client has cheated them. Meanwhile, the insurance company adds the unpaid service to its profit margin. The involvement of a third party in what is supposed to be a reciprocal relationship between two parties, one providing a service and the other receiving the service, creates a diffusion of responsibility; and when that third party is motivated by its profit margin to pay out less in services than its client pays in for services, a conflict of interest develops.
4. Moral Hazard
Related to diffusion of responsibility is the concept of moral hazard. When someone else (e.g., insurance company) is responsible for the risks (e.g., financial) another (e.g., client) incurs, the less responsible party (e.g., client) behaves differently than they would under maximum risk exposure (Wikipedia). For example, a teenager who buys his own car is more likely to take his ownership responsibility seriously, taking better care of the car, compared to a teenager whose parents buy him a car. Let’s consider how this is relevant in therapy. To begin, the financial responsibility for therapy isn’t felt by the client; they do pay for the service, but indirectly by paying for another service (i.e., insurance). The concept of moral hazard would say that the client would be more likely to take on financial responsibility they might not be able to afford if someone else is supposedly responsible. Further, if clients did bear the full, direct financial responsibility for therapy (by paying for services directly), they would not likely seek services unless they could pay for the services. By purchasing and utilizing insurance, clients are putting themselves in positions of financial vulnerability and are likely unaware that they are doing so.
5. Enlightened Self-Interest
The concept of enlightened self-interest also explains which party is most motivated to ensure a payment is made (Powers, 2017). When the insurance company won’t pay a claim and especially when the reason(s) for rejecting a claim is(are) pinned on the provider for allegedly not following the convoluted rules, who is most motivated to make sure the claim is paid: the provider, the insurance company, or the client? The party who is most motivated is the party who stands to lose/gain the most; that is the party who isn’t being paid for a service they already provided, the therapist. As a result, the therapist is highly motivated to spend additional time, fighting with the insurance company to try to get the claim paid. Further, if the insurance company refuses to pay the claim, asserting that the provider failed to follow an obscure rule, the client is exempted from their responsibility to pay for the service that they already directly received. Even if the insurance company does not blame the provider for the rejection, the client has little motivation to pay the claim, given that they have already received the service. The therapist is in a one-down position. Imagine the strain that this lack of reciprocity puts on the therapeutic relationship. Even if the client pays for the service that wasn’t covered by insurance, how are they going to feel, initially going into the relationship with the therapist, believing that all services will be covered by a third party, and then incurring a large bill? Who is the client going to be upset with? Perhaps their insurance company, but how about if the client has attachment problems? And, how about if the insurance company blames the provider for the insurance company’s refusal to pay the claim (e.g., “provider provided a service that was not medically necessary”)? And, what does this process communicate about who is responsible for the client’s care? Taking insurance doesn’t benefit the therapist, it benefits their client. Therapists are being paid less than their market rate (low as it already is), and they have to do a great deal of extra, unpaid work so their client can use their benefits. This isn’t fair to providers.
Not only does the concept of enlightened self-interest identify the party with the highest level of motivation to ensure that claims are paid, enlightened self-interest speaks to personal responsibility for recovery. Like the teenager who purchases his own vehicle, when people pay for something directly, they are more likely to be motivated to “get their money’s worth”, putting more time and energy into their investment. They now assume ownership of the service they have purchased and see recovery as their responsibility, as their recovery. When it appears that someone else is paying for the service (e.g., insurance company), even if this is a false perception, the level of ownership is diminished, as is level of responsibility for recovery.
Adding another layer of complexity to the impact of third-party payment for a service is the fact that when a third party pays for a service, that party assumes control over the type, amount, and frequency of the treatment because that party is paying for the service. That party is motivated to keep costs of services down to maximize profits. Curiously, in the case of health insurance, that party isn’t actually paying for the service, the client is, indirectly. Yet, the third party assumes control over care. By involving a third party in payment for mental health services, clients give up control over their treatment. The insurance company is not doing the client any favors by offering their health insurance service, and neither are therapists by accepting insurance. The client still pays for treatment, but has little control and ownership over their treatment and recovery. Is this a practice we want to perpetuate by continuing to accept insurance and following the treatment practices dictated by insurance companies?
6. Reciprocity
Even if all claims are paid without any problem, lack of reciprocity between client and therapist still occurs. According to Cialdini, the rule of reciprocation states, “…we should try to repay, in kind, what another person has provided us” (Cialdini, 2009, p. 19). How can a reciprocal relationship exist when one person provides a direct service and someone other than the person receiving the service pays for it? Further, what happens when that third party doesn’t pay for the service or pays a pittance for the service? When a relationship is not reciprocal, a power imbalance develops; in this case, it’s a power imbalance with the therapist in power and the client in a position of indebtedness. This type of dynamic is not only counterproductive but can be harmful in the context of any relationship, especially the therapeutic relationship. It places an already vulnerable individual in the position of increased vulnerability and leaves them open to exploitation. This is the antithesis of the dynamic we want to create in therapy.
D. The Future of Mental Healthcare Under the Third-Party Payer Model
1. Enabling the Harmful System to Continue
By credentialing with the insurance companies, and doing to the work to ensure that they pay for their clients’ services (because therapists want to get paid), therapists insulate their clients from their insurer’s devious behaviors, and they enable a harmful system to continue to exist. Consider this example, if a mother protects her children from their abusive father by taking the physical abuse herself, is she actually protecting them? No, she’s not. The way to protect her children is to get away from that man; that is the only way they can all be safe. Further, how able is she to help and protect her children when she’s being abused? Not very well. And, how able is she to change the dynamics that exist in that abusive situation and begin the healing process while she is still living in it? That will be a nearly impossible task and any therapist who works with her is going to focus on getting her out of there, not on trauma treatment. In fact, trauma treatment is contraindicated in situations where someone is actively being abused. Do you see where I’m going with this? If therapists don’t agree with the health insurance system and think it’s harmful to people, including themselves, then they need to get out. Therapists need to make changes from the outside and stop helping to support the system from the inside. Therapists are impotent to make changes when they are dependent on their abusive partner to pay their bills.
2. The Fall of Private Practice Under the Third-Party Payer Model
If therapists aren’t yet convinced that accepting insurance is not in their best interest or in their clients’ best interest, we should talk about the future of mental healthcare under the current insurance system. As discussed earlier, under this system, the medical field has been turned into a factory, and physicians into assembly line workers. The field of mental health is also turning into a factory, utilizing a Western Medical Model that pathologizes abuse, neglect, and other traumas and utilizes briefer, symptom-reduction-based treatments. Providers have been forced to abbreviate treatment, experiencing reductions in allowable treatment session length, treatment frequency, and treatment duration, with more reductions on the horizon. Ultimately, therapists are not able to practice according to best practices if they would like to receive insurance reimbursement.
It is my understanding that the plan is to phase out the smaller clinics and independent practitioners because it’s much more cost-effective to contract with one large clinic than many small clinics. Not only are there fewer contracts to write and manage, larger clinics are able to offer on-call services, which apparently cut down on inpatient hospitalizations, and ultimately, cut costs for insurance companies. Indeed, as mentioned earlier, insurance companies in the Twin Cities Metro area and Duluth have already begun to refuse contracting with new clinicians, unless they are part of a group contract with a larger clinic, so this phasing out process has begun. Additionally, to cut costs, insurers are rolling out therapy apps to cut down on costs of paying actual therapists, further pointing to the start of a phasing-out process. I could be wrong, but it looks to me like Rome is falling. And, as with the fall of the Roman Empire, the smart Romans left before it fell (Powers, 2017). My advice to therapists: When in Rome, leave before the Empire falls.
3. How Providers Can Evolve
As I discussed in the beginning there are many reasons therapists credential with insurance: 1) it’s what everyone does; 2) doing so ensures a steady referral stream; 3) it provides access to care to a wider demographic; an opportunity to “give back”; 4) they have skills deficits and fears that prevent them from converting to private pay such as A) “I don’t know how to market and run a business”; B) “Making money is bad”; “Providing charity is good”; C) “No one who buys insurance will pay extra to see me”; and D) “I’ll never find enough private pay clients to pay my bills”; “Some money is better than no money”. Even if this article has convinced therapists that it would be in their best interest and their clients’ best interest to get off insurance panels, raise their rates, and move to private pay, these rationale and fears will probably keep them stuck. So, I’m going to provide some suggestions to address each of these.
1) It’s what everyone does. I’m going to challenge you to challenge the status quo. It’s terrifying, trust me, I know. (I was terrified to write this article.) Courage is about being terrified but doing something anyway. If you aren’t already working with your own therapist, I’d encourage you to get a therapist and work on some of the fears you have surrounding challenging the status quo. (Shameless self-promotion: I can help you with this!)
2) Ensures a steady referral stream. If you learn how to market, you can develop a steady referral stream without being dependent on insurance. Begin networking with other small business owners who have been successful and get to know successful private pay therapists. There are a lot of really great free resources online that will teach you to market your therapy practice. There are also a lot of courses you can purchase, books you can buy, and/or consultants you can work with to help you learn to market. Further, many of the consultants offer free resources via podcasts, blogs and mini-courses. I’ve mentioned many of them below.
3) Provides access to a wider demographic; an opportunity to “give back”. I don’t believe that your business is necessarily the place to give back (or that you need to give back more than you already are as a therapist), but if it must be, please follow the airlines’ moto, “Secure your oxygen mask before assisting others.” Until you are in a place of financial integrity, it is not the time to give back. And when you are in a place of financial integrity and if you insist that you need to give back through your business, you can offer some sliding scale or pro bono spots. However, there are some dynamics that can play out when offering services for reduced rate or free, so please be aware (McLain, 2018). This also might be something helpful to work on with your individual therapist. And, I’ve included some books addressing financial integrity below.
4) Skills deficits and fears related to running a business get in the way. For the skills deficits, again, there are a lot of great, free resources and courses to help you learn to run a business (e.g., “Selling the Couch Podcast”); there are also some great courses you can purchase (e.g., “Abundance Practice Building”; “Your BadAss Therapy Practice”), books you can buy (e.g., Profit First; The Dip; The Millionaire Next Door; Your Money or Your Life) and/or consultants you can hire to help. Network with other successful professionals and figure out their methods. For the fears, I would specifically like to address the fear, “No one who buys insurance will pay extra to see me.” Yes, they will, and they are actually paying someone right now; that person is called their life coach. And, their life coach is charging them between $200-$667 per hour for a service you are fully capable of providing (Burza; Marver; Stimpson). As I mentioned before, working with an individual therapist will be helpful in overcoming your fears. Books such as Be a Wealthy Therapist, podcasts such as “The Practice of Being Seen” and courses such as Tiffany McLain’s “Lean In. Make Bank.” address many of these fears and provide opportunities and exercises for therapists to work through these fears.
If you, as a therapist, want to remove yourself from insurance panels and move into the world of private pay, it will be scary (terrifying) and will require learning some new skills, but it is possible. (This blog post provides a guide on how to terminate insurance contracts, including how to write a provider termination letter to insurance panels.) And, if therapists want to create a sustainable existence for ourselves, our clients, and our field, we have no choice but to evolve and make a paradigm shift. With any paradigm shift, there will likely be an upheaval and chaos as we all adjust to the new way, but such is the nature of challenging the status quo. The alternative to evolution is fairly undesirable.
Brianna Mann, Ph.D., works with protectors, caretakers, and high achievers in the Minneapolis, Minnesota area; and has been specializing in healing these individuals for over 16 years. She also works with therapists who want to leave insurance panels. Click to schedule an appointment or visit her website more information.
References
APA Center for Workforce Studies. (2015). 2005-2013: Demographics of the U.S. Psychology Workforce. Retrieved from http://www.apa.org/workforce/publications/13-demographics/index.aspx
Brandon, E. (2010, September 27, 2010). 5 Employers with Generous 401(k) Matches. U.S. News. Retrieved from https://money.usnews.com/money/retirement/articles/2010/09/27/5-employers-with-generous-401k-matches
Brekke, K. R., Holmas, T. H., & Straume, O. R. (2010). Margins and market shares: Pharmacy incentives for generic substitution. European Economic Review, 61, 1-38.
Burza, J. Jasna Burza Life Coaching. Retrieved from http://jasnaburza.com/life-coaching/
Cialdini, R. B. (2009). Influence: Science and Practice (5th ed.). Boston: Pearson Education Inc.
Edwards, H. S. (2017, August 15, 2017). What happens when doctors only take cash. Time.
Edwards, J. (2011). How pharmacists keep cash that could be yours on each generic prescription. Moneywatch. Retrieved from https://www.cbsnews.com/news/how-pharmacists-keep-cash-that-could-be-yours-on-each-generic-prescription
Frakt, A. (2018). Reagan, Deregulation and America’s Exceptional Rise in Health Care Costs. The New York Times. Retrieved from https://www.nytimes.com/2018/06/04/upshot/reagan-deregulation-and-americas-exceptional-rise-in-health-care-costs.html
Gold, J. (2017). If your insurer covers few therapists, is that really mental health parity? Kaiser Health News. Retrieved from https://khn.org/news/if-your-insurer-covers-few-therapists-is-that-really-mental-health-parity/
Government Accountability Office. (2011). Private Health Insurance: Data on Application and Coverage Denials. Retrieved from https://www.gao.gov/new.items/d11268.pdf.
Grunwald, M. (2018). Mulvaney requests no funding for Consumer Financial Protection Bureau. Politico. Retrieved from https://www.politico.com/story/2018/01/18/mulvaney-funding-consumer-bureau-cordray-345495
Hari, J. (2018). Is everything you know about depression wrong? The Guardian. Retrieved from https://www.theguardian.com/society/2018/jan/07/is-everything-you-think-you-know-about-depression-wrong-johann-hari-lost-connections?CMP=fb_gu
Health Partners Insurance. Health Partners Individual Plan. Retrieved from https://individualinsurance.healthpartners.com/hp/shopping/anonymous.html?&mode=&context=anonymous&_ga=2.87268824.1735581142.1527959113-934075219.1527959113 - view/productList/list
How to Become. How to Become a Dog Trainer. Retrieved from https://www.howtobecome.com/how-to-become-a-dog-trainer
Internal Revenue Service. (April 23, 2018). Self-Employment Tax (Social Security and Medicare Taxes). Retrieved from https://www.irs.gov/businesses/small-businesses-self-employed/self-employment-tax-social-security-and-medicare-taxes
Internal Revenue Service. (April 23, 2018). Understanding Employment Taxes. Retrieved from https://www.irs.gov/businesses/small-businesses-self-employed/understanding-employment-taxes
Kaiser Family Foundation. (2018). Professional Active Physicians by Gender. Retrieved from https://www.kff.org/other/state-indicator/physicians-by-gender/?dataView=1¤tTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
Kennedy, P. (2017, December 17, 2017). Nonprofit 100: Healthcare leads as we look at the top 100 nonprofits of 2017. Star Tribune. Retrieved from http://www.startribune.com/nonprofit-100/460547793/
Kennedy, P. (2018, April 20, 2018). CEO Pay Watch: Stephen Hemsley, UnitedHealth Group executive chairman. Star Tribune. Retrieved from http://www.startribune.com/ceo-pay-watch-stephen-hemsley-unitedhealth-group-executive-chairman/480423243/
Kirkham, E. (2017). Everything You Need to Know About Income-Based Repayment (IBR). Retrieved from https://studentloanhero.com/featured/income-based-repayment-plan/
Lazarus, D. (2017, January 17, 2017). How to fight back when an insurer denies your healthcare claim. Los Angeles Times. Retrieved from http://www.latimes.com/business/lazarus/la-fi-lazarus-winning-insurance-appeals-20170117-story.html
Marver, F. Begin Again Coaching. Retrieved from https://www.beginagaincoaching.com/ratesfaq
McKennon Law Group PC. (2017). How insurers deny legitimate health insurance claims. Retrieved from https://www.mslawllp.com/how-insurers-deny-legitimate-health-insurance-claims/
McLain, T. (2016). Ten myths therapists believe about setting fees. Retrieved from https://www.heytiffany.com/top-10-myths-therapists-have-about-setting-fees/
McLain, T. (Producer). (2018, March 2, 2018). Lean In. Make Bank. [Online Course] Retrieved from https://www.heytiffany.com/lean-in-make-bank/
Miller, K. (2016). The Simple Truth About the Gender Pay Gap. Retrieved from https://www.aauw.org/research/the-simple-truth-about-the-gender-pay-gap/
Organisation for Economic Co-operation and Development, O. (2015). Health at a Glance 2015: How does the United States compare? Retrieved from https://www.oecd.org/unitedstates/Health-at-a-Glance-2015-Key-Findings-UNITED-STATES.pdf.
Universal Underwriters Ins. Co. v. Travelers Insurance Co. , 451 S.W.2d 616, 622-623 C.F.R. (1970).
PayScale. Salary Data & Career Research Center (United States). Retrieved from https://www.payscale.com/research/US/
Pelley, S. (Writer). (2014). Denied: When insurance companies deny the mentally ill the treatment their doctors prescribe, seriously ill people are often discharged, and can be a danger to themselves or others. In M. Rey & O. Zill-de Granados (Producer).
Powers, B. (2017, July 12, 2017). [Personal Communication].
Powers, B. (2018, June 6, 2018). [Personal Communication].
Rubin, E. (2010, May 17, 2010). Is the training of a psychiatrist more like that of a neurologist or a psychologist? Retrieved from https://www.psychologytoday.com/us/blog/demystifying-psychiatry/201005/is-the-training-psychiatrist-more-neurologist-or-psychologist
Schoen, D. (2017, August 15, 2017). Too many Americans with insurance are being denied health. The Hill. Retrieved from http://thehill.com/blogs/pundits-blog/healthcare/346652-too-many-americans-with-insurance-are-being-denied-coverage)
Smart Asset. Federal Income Tax Calculator. Retrieved from https://smartasset.com/taxes/income-taxes - jHNjpDIYGo
Stimpson, M. Lifeshine Coaching. Retrieved from https://www.lifeshinecoaching.com/)
Study.com. Insurance Broker Education Requirements. Retrieved from https://study.com/articles/Insurance_Broker_Educational_Requirements_to_be_a_Licensed_Insurance_Professional.html
Study.com. Investment Banking Education Requirements and Career Info. Retrieved from https://study.com/investment_banking_education.html
Study.com. Requirements to become a doctor in the U.S. Retrieved from https://study.com/requirements_to_become_a_doctor.html
Tandon, A., Murray, C. J., Lauer, J. A., & Evans, D. B. (2000). Measuring overall health system performance for 191 countries. Retrieved from http://www.who.int/healthinfo/paper30.pdf
Truffo, C. (2007). Be a Wealthy Therapist: Finally, You Can Make a Living Making a big Difference. Saint Peters, Missouri: MP Press.
U.S. Inflation Calculator. Retrieved from http://www.usinflationcalculator.com/
Wikipedia. Coaching: Life coaching. Retrieved from https://en.wikipedia.org/wiki/Coaching - Life
Wikipedia. Moral Hazard. Retrieved from https://en.wikipedia.org/wiki/Moral_hazard
Wikipedia. Nonprofit organization. Retrieved from https://en.wikipedia.org/wiki/Nonprofit_organization
Willyard, C. (2011). Men: A growing minority? gradPSYCH Magazine.
Endangered Species: Homo Sapiens
Technology and our blindness to its ramifications have placed mankind on an unknown trajectory advancing at the speed of light; if we do not slow down long enough to consider our destination, we may unwittingly and prematurely become faced with our own mortality (metaphorically, if not literally). Virtual reality has become a playground for anonymity, dissociation, and the whims of the id. Our legal system is severely lagging behind the savvy of virtual crime and psychology is poorly equipped to face the changing dynamic of the way its consumers interact.
Technology and our blindness to its ramifications have placed mankind on an unknown trajectory advancing at the speed of light; if we do not slow down long enough to consider our destination, we may unwittingly and prematurely become faced with our own mortality (metaphorically, if not literally). Virtual reality has become a playground for anonymity, dissociation, and the whims of the id. Our legal system is severely lagging behind the savvy of virtual crime and psychology is poorly equipped to face the changing dynamic of the way its consumers interact.
Self becomes more anonymous and thus, unrestrained. Self becomes anything we want it to be and this instability of self is not judged mentally disordered. Current society devotes so much time to discovering the true self and places tremendous value on finding the answer. Do we realize that through interaction with the virtual world, we are undoing what we are seeking, perhaps even as we are seeking it? Many of us long to again entertain the fanciful world of childhood make-believe, but know this will lead to certain scorn. The virtual world allows us to be someone else for a short period of time and to escape the doldrums of everyday life. This does not necessarily create a problem until individuals begin to abandon real life for the virtual or begin to take risks they would never consider in the physical world (e.g., giving your address and personal information to a virtual friend/real-life stranger). Has a society generally devoid of real-world risk led us to create our own risk for entertainment value via shifts in virtual self and risky behavior in the virtual world?
Action and actor are becoming dissociated. Do we view the man who murdered someone with his bare hands similarly to the man who pushes a button to launch a missile? Technology has enabled this disconnect between not only actor and action but between actor and responsibility. How does the court system handle cyberbullying versus face-to-face bullying and how do we treat these behaviors in therapy? Certainly, individuals in both scenarios are culpable but as therapists, we may have more difficulty convincing one of a more abstract level of responsibility than a concrete, behavioral level of responsibility. Challenging maladaptive overt behavior is a much more objective endeavor than challenging attitudes, cognitions, and covert or virtual behavior. Indeed, the theory of cognitive dissonance states that when faced with discordant behaviors and attitudes, we are more likely to change the attitudes because they are more malleable, whereas behavior is overt and more difficult to rationalize or change post facto. What implications does this theory hold for virtual “behavior” or behaviors conducted by a remote actor?
Virtual therapy may be the wave of the future. The internet application called “Second Life” allows you to create a virtual world with a virtual self, an avatar. Prominent therapists have proposed setting up accounts in Second Life to train new cognitive therapists and eventually even conduct therapy. Though this sounds a bit far-fetched, therapists in rural areas are already implementing and evaluating the efficacy of remote therapy via teleconference. Obviously, the remote therapy dynamic is not ideal for purposes of safety and rapport building, but in many cases, this may be some individuals’ best chance at receiving optimal services or any services at all. Despite concerns regarding physical disconnect between mental health professional and client, if psychology does not keep up with current technology, “therapeutic” resources in these forms are sure to spring up elsewhere and will certainly be utilized by consumers for convenience sake (e.g., therapy apps). We are a pill-popping, fast-paced, action-oriented society who wants to see the fruits of our labor, yesterday. We don’t have time for face-to-face appointments, grueling standardized testing procedures, waiting lists, or in-depth, long-term therapy. If psychology does not change to face societal demands, it will become as antiquated as our old friend, the telegraph. The paradox is, if psychology changes to prevent extinction, we risk losing the magical parts that make it work (e.g., the feeling of connectedness you can only feel by being in the presence of another human who is fully engaged in what you are experiencing).
The obvious consequences of a shift from actual identity to virtual identity are terrifying: greater anonymity, a changeable self, dissociation from act and actor as well as diffuse sense of responsibility. The popular press has elucidated some of the problems already caused by such identities as well as our lack of preparedness for addressing the ramifications. More terrifying, are the consequences that have yet to manifest themselves and the consequences that we will be unable to predict. Through our own doing, we appear to have created a personality-snatching monster. Perhaps the quandary facing us is not where we will be in 50 years, but what we will be.
Note: I originally wrote this essay on 05.07.09 as a course assignment while I was a Ph.D. student. I thought it would make a timely blog post, over 8 years later with a vastly changed social media landscape. The YouTube video below, featuring former Facebook executive Chamath Palihapitiya, brings my concerns into present day focus.
Brianna Mann, Ph.D., works with protectors, caretakers, and high achievers in the Lake Minnetonka, Mound, and St. Louis Park, Minnesota areas; and has been specializing in healing these individuals for over 15 years. She also works with therapists who want to leave insurance panels. For more information, please see www.briannamannphd.com